7 Minute Read
Recently, simulation expert Professor Gerry Gormley shared that he had renamed his simulation debriefing room the
Learning Conversation Room

The name change is subtle, but it struck me as a powerful reframing. At a recent simulation symposium in Sydney, Professor Walter Eppich and Nathan Oliver challenged the common tendency to place “debriefing”, “coaching” and “feedback” into separate conceptual boxes, as though they are entirely distinct educational activities.
They are all forms of Learning Conversation.
In practice, these 3 types of Learning Conversation (pictured) can overlap.
An important question may not be which box a conversation belongs to, but what kind of learning we are trying to support.

At times, we have historically placed feedback, coaching and debriefing into rigid conceptual boxes, treating each as a discrete practice and overlooking the ways they can productively intersect.
In more recent times, we increasingly blur the boundaries, using the terms loosely and interchangeably within our different workplace learning cultures.
On the one hand, clearly when we are learning about ‘Feedback’ for the first time seperating the contructs out and applying some rules is a good idea. The types of conversation at their roots have distinct purposes, postures and emphases, but in practice they frequently overlap.
However, in my view (and Walter and Nathans presentation’s view) there is increasingly blurred boundaries and overlap. Understanding the overlaps and differences can help us become more deliberate educators and perhaps create richer learning cultures in our workplaces.
Therefore, our task is not to defend the boundaries between them, nor to pretend that those boundaries do not exist, but to understand what each approach offers and to use it deliberately in response to the learner and the team at a given moment.
Examples of Overlap
A debriefing may contain elements of feedback or ‘providing information’
Future focussed coaching elements may be used naturally during a debriefing.
Feedback conversations frequently conclude with coaching questions and action plans.
Feedback: Understanding the Gap
Feedback has been one of the most studied concepts in medical education, yet it remains one of the most misunderstood.
Traditionally, feedback has been viewed as information provided to a learner about their performance. Molloy and colleagues describe feedback as:
“A process whereby learners obtain information about their work in order to appreciate the similarities and differences between the appropriate standards for any given work, and the qualities of the work itself, in order to generate improved work.”
This definition moves beyond the simplistic notion of praise or criticism. Effective feedback is not about making people feel good or bad. It is about helping learners understand the gap between current performance and desired performance, so that future performance can improve.
The classic feedback cycle remains remarkably persuasive. Practice generates performance. Feedback informs reflection. Reflection guides improvement. Improvement drives further practice.
Without feedback, deliberate practice risks becoming repetition. Without practice, feedback becomes little more than an interesting conversation.
Yet despite decades of effort devoted to teaching educators how to “give better feedback”, learners continue to report dissatisfaction with both the quality and quantity of feedback they receive. This has prompted a shift in thinking away from feedback as a delivery process and towards feedback as a shared educational activity.
The concept of feedback literacy reflects this evolution. Feedback literacy recognises that learners must actively participate in feedback processes. They need to appreciate the value of feedback, judge their own performance, manage emotional responses and translate insights into meaningful action. Receiving feedback effectively is itself a learned skill.
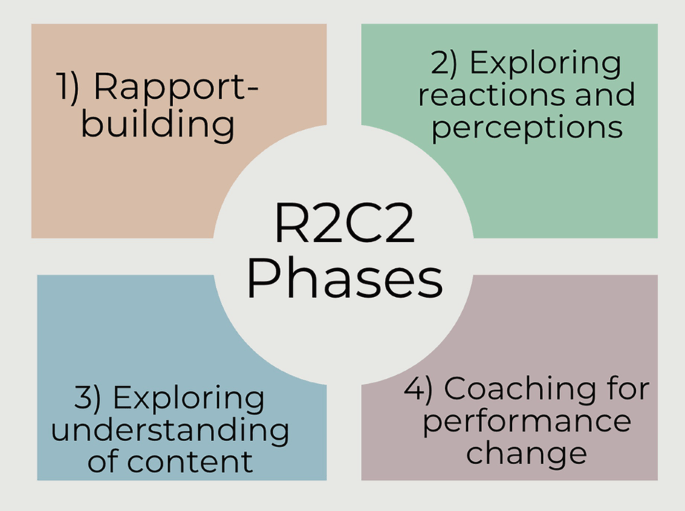
Similarly, frameworks such as the R2C2 model (Relationship, Reactions, Content and Coaching) have moved feedback away from a one-way transmission model and towards dialogue. Feedback becomes a conversation rather than a monologue. Relationship comes first. Reactions are explored before performance data are discussed. Most importantly, the process concludes with coaching and future planning.
This progression highlights an important reality: feedback alone is rarely enough. Understanding a gap does not automatically close it.
Coaching: Unlocking Future Performance
If feedback is primarily concerned with understanding performance, coaching is primarily concerned with developing potential.
The distinction is subtle but important.
Feedback often looks backwards. Coaching looks forwards.
Feedback may answer the question, “How did I do?”
Coaching asks, “What could I become?”
The coach adopts a different posture from the feedback provider. Rather than evaluating performance, the coach seeks to facilitate reflection, promote agency and support the learner in identifying their own solutions.
One of the most widely used coaching frameworks is the GROW model:
- Goal – What do you want to achieve?
- Reality – Where are you now?
- Options – What possibilities exist?
- Way Forward – What will you do next?
Notice how little of the framework requires expert opinion. The coach’s role is not necessarily to provide answers, but rather to create the conditions in which learners can generate their own.
This future-focused orientation often makes coaching feel empowering. The conversation emphasises strengths, possibilities and growth. Rather than concentrating on deficits, coaching seeks to expand capability.
Of course, coaching is not the absence of challenge. Effective coaches frequently ask difficult questions. However, the challenge emerges through inquiry rather than judgement. However, the learner remains firmly in the driver’s seat.
Debriefing: Making Sense of Experiences
Debriefing occupies a subtley different space again.
Where coaching is often future-focused and individualised, debriefing is commonly anchored to a shared experience. The purpose is not simply to improve future performance, but to help participants make sense of what has happened.
This is particularly relevant in simulation, emergency medicine, critical care and other high-acuity environments where teams must process complex events together.
A debriefing may explore:
- What happened?
- Why did it happen?
- What were people thinking?
- What influenced their decisions?
- What can be learned from the experience?
Unlike coaching, debriefing often focuses on both performance and cognition. It seeks to uncover mental models, assumptions, situational awareness and decision-making processes. The discussion may move beyond the individual and into team dynamics, systems factors and organisational influences.
Psychological safety remains essential, but safety should not be confused with comfort or ‘easy’.
An effective debriefing may involve elements of challenge or critique. It may include observations about performance that closely relate to real-life healthcare pratice. Facilitators may teach, guide, challenge assumptions or identify problematic behaviours. Judgement is not necessarily absent; rather, it is used carefully and transparently in service of learning.
This is one reason why debriefing often feels fundamentally different from coaching:
Coaching asks learners where they want to go.
Debriefing helps learners understand where they have been.
The Boundaries are Blurry
In reality, the boundaries between these conversations are far from rigid.
An emergency department resuscitation debrief may begin with collective reflection, transition into feedback about communication, and conclude with coaching questions about leadership development.
Similarly, simulation methodologies such as Rapid Cycle Deliberate Practice (RCDP) intentionally blend educational approaches. The pause-and-repeat model incorporates immediate feedback, coaching prompts, micro-debriefs and deliberate practice in rapid succession.
Experienced educators move fluidly between these approaches depending on learner needs and contextual demands but also recognise the important of culture.
Building the Culture
Professor Christopher Watling’s influential work suggests that many of medicine’s feedback challenges are not primarily technical problems – they are cultural ones.
In another a fascinating study involving physicians who were also accomplished athletes and musicians, Watling and colleagues found that effective feedback shared similar characteristics across domains. Good feedback was specific, credible and actionable regardless of context. What differed was culture.
Learning cultures influenced expectations of teachers, expectations of learners and norms surrounding feedback itself. In music and sport, feedback was normalised. Observation was expected. Performance critique was routine. Improvement was understood as an ongoing process rather than an occasional event. Medicine often struggles to achieve the same norm.
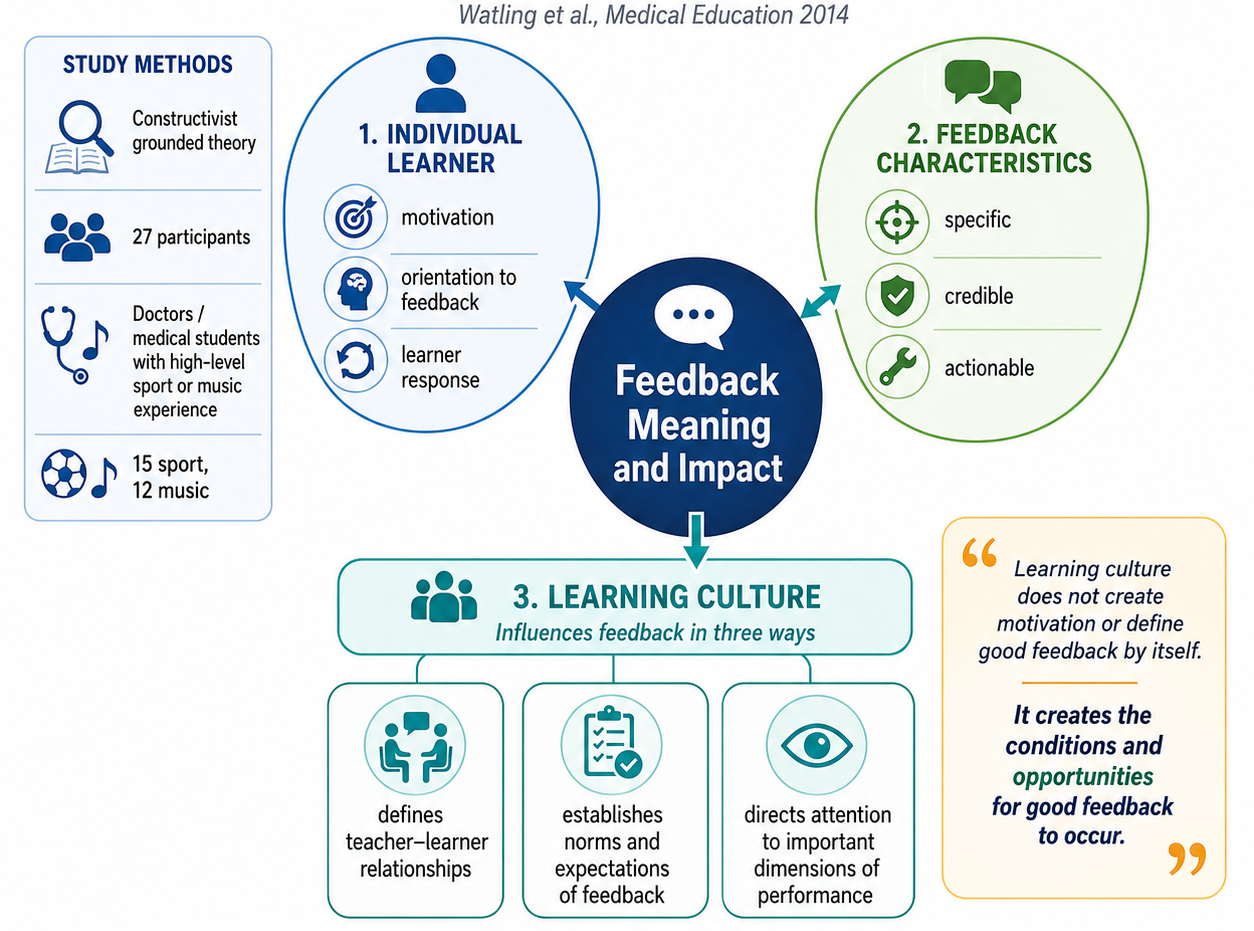
As the prolific Watling argues, learning culture does not create motivated learners, nor does it define good feedback. Instead, culture creates the conditions under which good feedback can occur and under which learners can meaningfully engage with it.
Perhaps the same could be said of coaching and debriefing. The goal is not merely to master a framework or adopt a particular conversational model. The goal is to create environments where learning conversations are expected, valued and psychologically safe. In environments (such as music) where observation is normal, curiosity is encouraged and improvement is celebrated.
Whether we call them feedback conversations, coaching conversations or debriefings may matter less than the culture in which they occur. Each has a distinct purpose, posture and emphasis, but their educational value depends on whether learners experience them as routine opportunities for growth or as moments of threat and judgement.
The fact that the phrase, “Can I give you some feedback?”, still provokes trepidation in many healthcare learners should concern us. It suggests that feedback remains culturally associated with deficiency, correction and assessment rather than with observation, dialogue and improvement.
Conclusion
Watling and colleagues remind us that learning culture shapes expectations, relationships and the meaning learners attach to feedback. A healthy learning culture does not make every conversation comfortable, but it makes learning conversations expected, credible and useful. It normalises feedback, builds trust, clarifies performance goals and aligns teachers and learners around a shared purpose: getting better.
Perhaps that is why the idea of a Learning Conversation Room resonates so strongly.
And perhaps the most important task for health professions educators is not becoming better at feedback, coaching or debriefing in isolation. It is creating conditions that positively infuence the culture in which all three can flourish.
References
- Molloy E, Boud D. Feedback models for learning, teaching and performance. In: Delany C, Molloy E, editors. Clinical Education in the Health Professions. Elsevier; 2018.
- Molloy E, Boud D, Henderson M. Developing a learning-centred framework for feedback literacy. Assessment & Evaluation in Higher Education. 2020;45(4):527–540.
- Sargeant J, Lockyer J, Mann K, et al. Facilitated reflective performance feedback: developing an evidence- and theory-based model that builds relationship, explores reactions, examines content and coaches for performance change (R2C2). Academic Medicine. 2015;90(12):1698–1706.
- Whitmore J. Coaching for Performance. 5th ed. London: Nicholas Brealey Publishing; 2017.
- Eppich W, Cheng A. Promoting excellence and reflective learning in simulation (PEARLS): development and rationale for a blended approach to healthcare simulation debriefing. Simulation in Healthcare. 2015;10(2):106–115.
- Sawyer T, Eppich W, Brett-Fleegler M, Grant V, Cheng A. More than one way to debrief: a critical review of healthcare simulation debriefing methods. Simulation in Healthcare. 2016;11(3):209–217.
- Cheng A, Hunt EA, Donoghue A, et al. Examining pediatric resuscitation education using simulation and deliberate practice: a review of Rapid Cycle Deliberate Practice. Resuscitation. 2020;152:37–44.
- Watling C, Driessen E, van der Vleuten CPM, Lingard L. Learning culture and feedback: an international study of medical athletes and musicians. Medical Education. 2014;48(7):713–723. Full Text – Click Here
- Watling C. Building a feedback culture. Keynote presentation, Health Professions Education; Western University, Canada.
- Watling C, Ajjawi R, Bearman M. Approaching feedback as a learning culture rather than a teaching technique. Medical Education. 2022;56(9):885–888.
