
UPDATED PAGE UPDATED 7th August 2026
WOUND CARE WORKSHOP NOTES:
https://docs.google.com/document/d/17ra6ttSbYV14aUxnmBtq32l1hTwosyltW-ufg8XdyOU/edit?usp=sharing
Blog Post
In the Emergency Department (ED) most wounds are closed by the ‘in-house’ medical and trained nursing staff (NPs).
However, a number of wounds should not be closed either “at all”, in the case of some human and animal bite wounds, or “not in ED but in theatre”. At the outset this should be considered a key question in the decision making process when the patient presents to the Emergency Department.
Hospital resources (e.g. surgical team, plastics and ED staffing rations), location of the department and a variety of time factors may determine the appropriateness of full management of a wound in the ED setting.

Compound fractures and injuries involving vital structures such as tendons, arteries and nerves are examples of wounds that require referral to specialist teams such as plastics, max-fax surgery, opthalmology, orthopaedics and general surgery. In sum, before repairing or suturing a wound such as a laceration we should make an adequate clinical assessment of the patient’s injury.
This assessment of an ED patient is outlined:
History
Ask the patient about (and document) all the events leading up to the injury
Mechanism is important, for example was this a Cat or Dog Bite?
These injuries are associated with a high risk of infection:

Was the injury caused by a sharp cutting object?
A cut from sharp implement is correctly termed an ‘incised wound’.
A true laceration is caused by ‘tearing’ from blunt trauma.
Take note of any allergies, past medical history and medications.
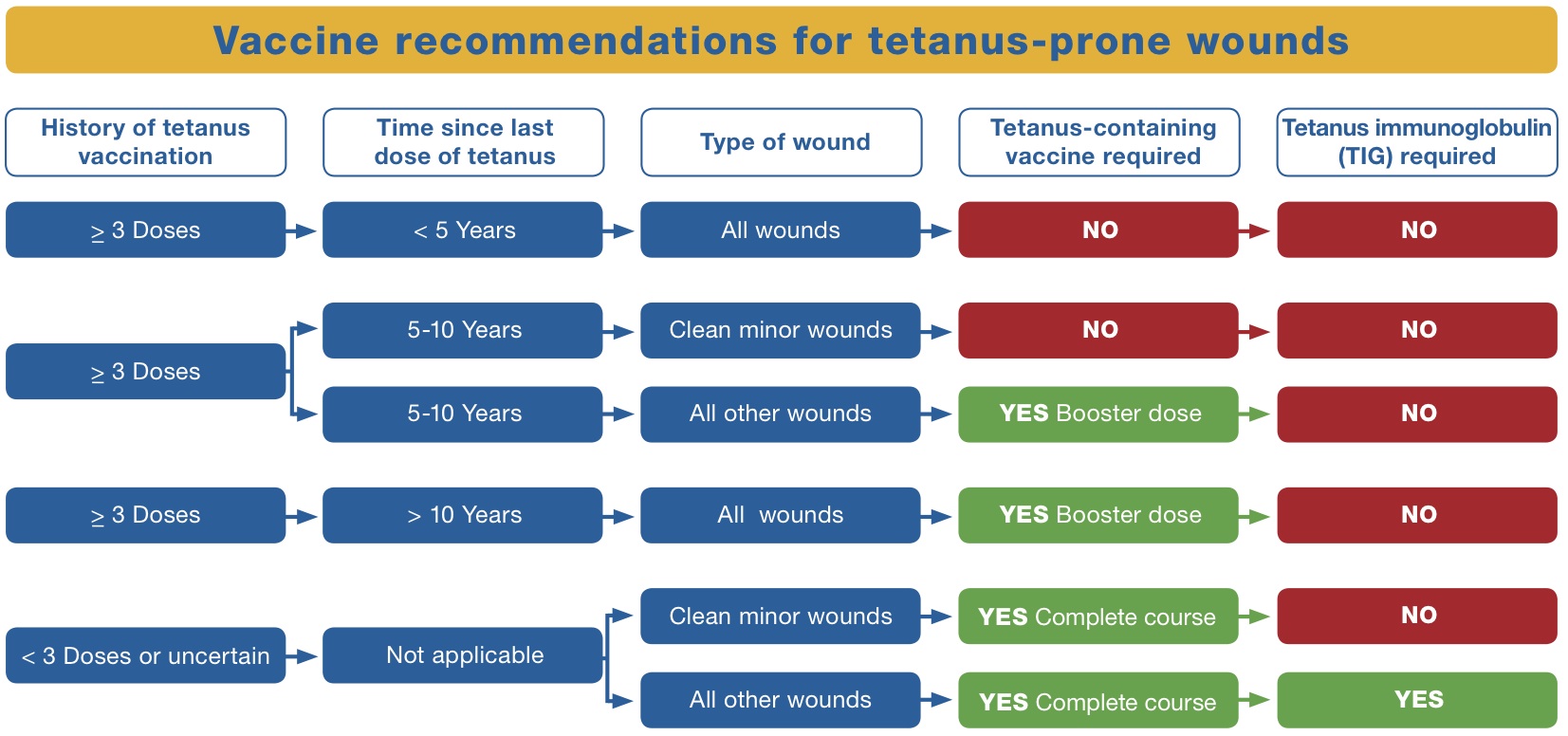
It is important to ask about Tetanus status (update the patients tetanus as per your Local Guidelines).
A patient Fact Sheet can be useful here.
Ask – Is there likely to be a Foreign Body?
Examination
General Inspection
Where is the Wound?
How deep?
How long? (Note this description in the medical record)
Use pictures where possible to add to your notes fidelity
What is the Neurological Function of the area affected?
For example is there any change in sensation?
Is the motor function of the limb normal?
Is there any evidence of Vascular Injury?
Are the Tendons intact or compromised?
Is there need for an X-ray for Foreign Body?

Is the wound contaminated? (wood, soil, rabies risk)
Be especially cautious with delicate wounds – always have a low threshold for a second opinion on wounds to areas such as the hand and face.
General Management of Wounds in the ED
Consent for further exploration and examination using local anaesthetic +/- closure of the wound
Gather Equipment
Wound Preparation
Anaesthesia (use no more than 3-5mg per Kg Lignocaine. 1ml 1% = 10mg)
Wound Clean (use Saline or Chlorhexidine)
Debridement and Examination
Further Copious Irrigation (use Saline) – Use a 14 cannula (plastic part) and 20ml syringes to achieve this effectively

Close wound as appropriate
Update Tetanus Immunisation
Wounds NOT to Close in the ED
Some Lip Injuries that are crossing the Vermillion border
Wounds with involvement of Vital Structures such as arteries, nerves and tendons
Severe Dental Injuries
Deep Wounds (e.g. involving muscle)
Penetrating Wounds
Heavily Contaminated Wounds or Wounds with Foreign Bodies
Compound Fractures
Bites (see below) – use antibiotics
NB – all of the above injuries require good basic wound care. This may include a primary ED closure after taking advice about management and follow up.
Wound Closure
Basically, with any given wound during the in the healing process it tends to contract over time. With our suturing we want a slight Eversion (because wounds will tend to contract back down to a neutral position).
Although most wounds can be sutured in the ED there are many wounds that we should not be closing (see above)
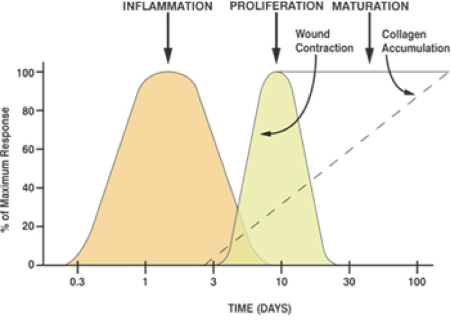
Wounds may be closed by primary closure (primary intention), delayed primary closure or left to heal by secondary intention. By any of these means the wound healing process is a dynamic one. It can be divided into three phases.
The phases of wound healing are:
- Inflammatory phase
- Proliferation phase
- Maturation phase
Simple Interrupted Sutures
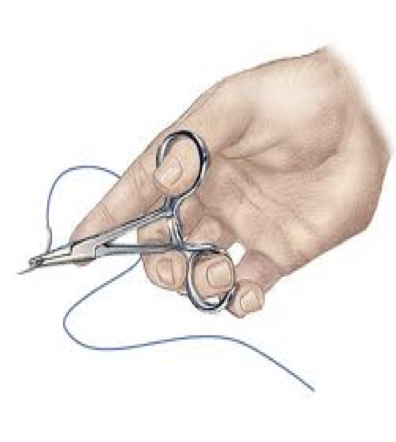
This is the mainstay for simple closure of wounds in the ED. Essentially the procedure is done with a run of interrupted sutures using instruments and basic knots. Using two hands the needle is carefully inserted through the skin and knots are tied in opposite directions (e.g. 2 throws in each direction). The aim is to mildly evert the wound to allow for contraction during healing. This is done by taking adequate accurate bites of cutaneous tissue and applying moderate tension to the sutures.


Correct Grip for Simple Suturing
Alternative Methods of Closure
Always consider alternatives whether an alternative method may be appropriate for closure. These options are available in most EDs. Ask a senior or nursing staff about these options if you are not sure where they are kept:
- Tissue Glue
- Staples
- Steristrips
Other Suture Techniques
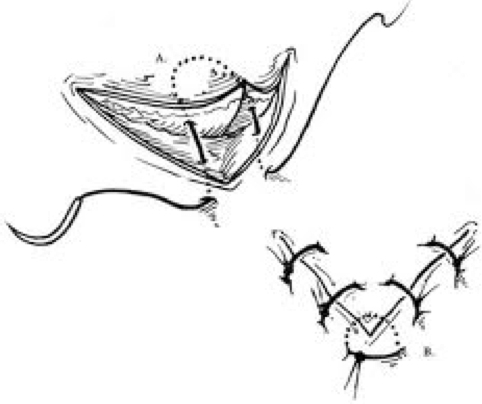
The techniques for a Mattress suturing are shown below. Mattress sutures create increased wound eversion and tensile strength. This can be useful for the refractory bleeding wounds and complex wounds that are seen in the ED. The downside to a mattress technique is the worsening of cosmetic results.
The ‘horizontal mattress’ is most commonly used in ED. This suture technique can be thought of as ‘Out–Out–In–In’ in terms of the order of bites taken:

Wound flaps and jagged edges can be neatly closed using a horizontal mattress technique:
Hand Ties – Two Handed
Hand Ties – One Handed
Continuous Interlocking Sutures
Continuous Suture techniques are quick with practice and can provide additional tensile strength in two directions when compared with interrupted sutures.
Running sutures (continuous sutures) have also been shown to reduce pain after episiotomy repair in large meta-analyses of controlled trials.
The Aftercare of Wounds
Aftercare of wounds is as important as assessment and closure.
We should consider appropriate dressings, in particular antibiotic paraffin (e.g. ‘Bactigras’). Some clinicians advocate the use of Chloramphenicol ointment around the wound. The sutures should generally be taken out within 1 week, and probably between 3 and 5 days for facial and delicate wounds. Wounds should be elevated to minimise swelling and advice given about keeping the wound covered and dry.
Usually the local GP should do a wound check and remove the sutures.
If there are particular concerns you can bring patients back to ED or ask them to see their GP after 2 days. One of the most important pieces of advice to give is in regard to sun protection. Exposure to sun in the first 1-2 months increases scarring. Therefore, advice the patient about sun block application.
Patients with chronic disease are at higher risk of ‘poor wound healing’. Diabetics should pay special attention to optimising their blood sugar and you should have a low threshold for reviewing these patients at an early stage.
Types of Suture
There are many types of suture material available. 3.0 Non-absorbable is a good suture to practice with and use in most simple wounds.
In medicine we often talk about ideals (e.g. the drug that cures everyone with no side effects). We propose that the ‘Ideal Suture’ would be Cheap, Easy to Handle, Provide an Optimum Balance between Tensile strength, Elasticity and Stay in Place, have Minimal Tissue reaction and have a Tailored Absorption Rate. This suture doesn’t exist so the selection of suture material depends on play off between the different types of suture material’s Pros and Cons.

TYPES OF SUTURE
Points on Selecting Suture Type:
Absorbable or Non-Absorbable
Either probably ok for simple skin sutures in the ED
Monofilament or Braided
Important in regard to strength
Braided sutures provide better knot security
Monofilament sutures provide better passage through tissue and produce less tissue reaction
Dyed or Undyed
Important in regard to ‘seeing’ sutures
Synthetic (e.g. Vicryl Polyglactin) or Non Synthetic (e.g. Silk, Cat Gut)
Most sutures today are synthetic
Fast absorbing gut is useful for oral and intestinal suturing
Cost – may be a consideration from an ED administration point of view
Types of Needle
Needles are generally divided into:
(1) CUTTING (‘Reverse and Conventional)
(2) TAPER (these are friable: ‘Non Cutting’ to minimise tissue damage)
Suture Anatomy
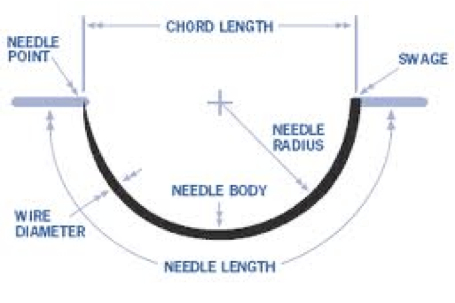
‘Reverse’ type sutures are the most commonly used in most Emergency Departments.
This type of suture gives optimum control of the depth of suture to the operator.
Thinking about size is also a consideration. A small needle will easily bend/break but will be superior for fine work and cause less tissue reaction if handled with care.
Size of your Suture: Very Large – Large – Medium – Fine – Micro
Gauge: 4 3 2 1 (0) 1/0 2/0 3/0 4/0 5/0 6/0 7/0
Conclusions
In summary, wound care in the ED is a common and important task. All wounds presenting to the ED require a thorough assessment and consideration for the most appropriate wound care in the ED.
Suturing requires practice and patience, where in doubt ask a colleague for assistance and always document your management and decision making process carefully in the medical record.
