PRINTABLE HANDOUT PDF DOWNLOAD

Automated Cardiopulmonary Resuscitation
Mechanical CPR
Good quality cardiopulmonary resuscitation (CPR) may improve cardiac and neurologic outcomes following cardiac arrest and this can theoretically be facilitated by various Mechanical CPR Devices that we will look at in this discussion. Early CPR has been associated with increased survival and is therefore very important in the ‘chain of survival‘ following cardiac arrest. For example, studies in the 1980s and 1990s suggested significant benefit from early bystander CPR and large observational studies in Japan have shown that compression only CPR may be favourable in adult cardiac arrest patients. These studies have begun trends towards widespread public health promotion of hands only CPR:
Hard and Fast
Push Hard – Push Fast
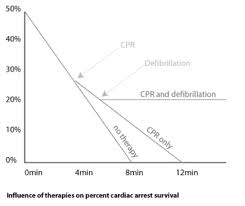
The chain of survival (shown below) emphasises the key steps in attempting to achieve an improvement in the currently low rates of survival in sudden cardiac arrest.
The chain of survival includes recognition (and calling for help), early CPR, early defibrillation and expert post resuscitation care including angioplasty therapy in the catheter lab.
Disappointingly, overall mortality rates have only marginally improved in the last 10 years despite rollout of public education, training of healthcare professionals and improvement in emergency medical systems. On-going discussion of how to improve survival from cardiac arrest is an important public health issue.

Phases of CPR
It can be helpful to think of CPR in 3 distinct phases:
- Phase 1 – The Electrical Phase – an early shock should result in a Return of Spontaneous Circulation (ROSC) in patients with Ventricular Fibrillation (VF).
- A Key concept in the “Chain of Survival”
- Principle behind early defibrillation (and precordial thump) in witnessed arrests in hospital
- DC shock should be administered as early as possible here
- The basis behind the widespread uptake of Automated Electrical Defibrillators (AEDs) in the out of hospital setting
–
- Phase 2 – The Circulatory Phase – effective CPR will theoretically “prime the pump”.
- Good quality (early) CPR is more likely to result in a Return of Spontaneous Circulation (ROSC).
- Patients with ‘non shockable’ rhythms such as Pulseless Electrical Activity (PEA) and Asystole start in this phase.
- This is the principle behind the emphasis on good quality CPR in the updated International Liaison Committee on Resuscitation (ILCOR) recommendations for resuscitation from 2010.
- Several shocks may be required to revert VF.
- Drugs may be helpful (at least in theory) to obtain ROSC.
- Phase 3 – The Metabolic Phase – things ‘look really bad’ now!
- There is a low chance of Return of Spontaneous Circulation (ROSC) due to accumulation of metabolic abnormalities.
- There is ischaemia and cell death associated with prolonged hypoperfusion and a progressive severe metabolic acidosis.
- End Tidal CO2 if often in the refractory low range (<10). Specific patient groups are more likely to survive (hypothermia and toxicology).

Automated CPR Machines
Automated CPR machines were introduced in the 1990s and have been used in limited clinical practice since then.
There are three main ways to deliver CPR – conventional manual compressions, pneumatic piston devices (i.e. Michigan® and Lucas®) and battery powered band compression machines (i.e. Zoll AutoPulse®)
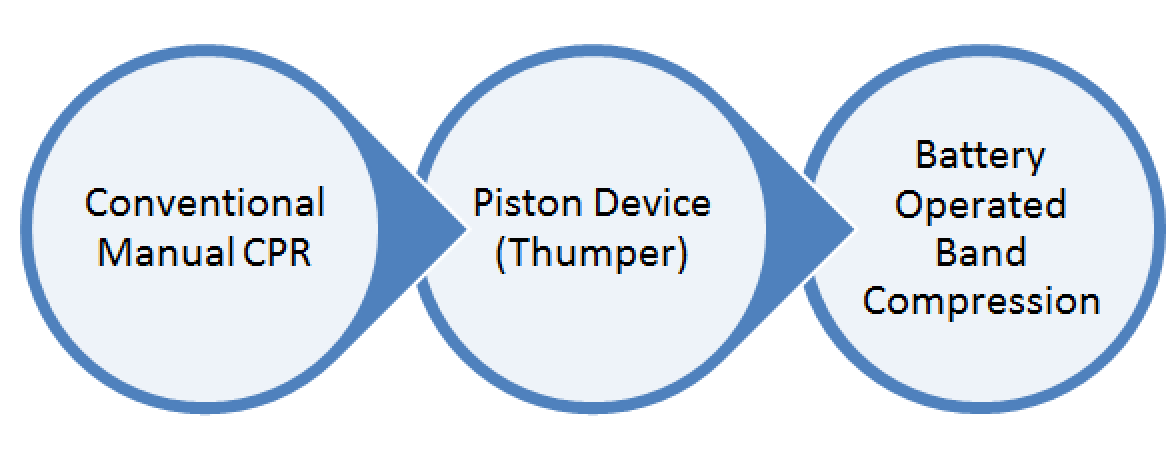
Automated CPR machines (‘thumpers’ and ‘band’ types) can provide consistent, good quality uninterrupted chest compressions. They have the potential to improve outcomes in sudden cardiac arrest and may ‘buy time’ if used early in appropriate patients.
What is the Evidence Base?
There is some good evidence for increased efficiency in experimental and animal studies but to date there has been a lack of high quality clinical studies demonstrating an overall mortality benefit. In fact, historically, results have been quite mixed with a landmark edition of JAMA in 2006 having two conflicting studies. One study (that was stopped early) showed a trend towards worsening outcomes with mechanical CPR and another study in the same issue suggested a potential benefit from a similar intervention.
Interestingly, in another negative study a year earlier called ASPIRE there appears to have been significant study protocol issues. In the ASPIRE study there was trending towards harm from using the Zoll AutoPulse and the research was subsequently terminated after an interim analysis. However, in the ASPIRE study there was a significant delay in applying the mechanical device in several patients in which time no active CPR was given. One study centre recorded >10mins of delay to apply the device in most cases which may have worsened outcomes significantly in the mechanical CPR group. Although the study was stopped early, later analysis suggested that this may have been due to protocol errors at one particular site rather than a truly harmful effect from mechanical CPR.
Provisional Results of the “CIRC” Trial are now undergoing scrutiny having been presented at various conferences.
Potential Benefits of Mechanical CPR
- CPR is a challenge in during transport – especially in a moving ambulance.
- Defibrillation success is dependent on maintenance of an adequate circulation (e.g. ‘circulatory phase’ above)
- Safety for staff
- Injury of rescuers from exertion or being thrown in the motor vehicle
- Minimising CPR rescuer tiredness
- Free up rescuers to do other tasks (cannulation, airway, handover)
- Consistent chest compressions (e.g. no fatigue factor)
- Continuous chest compressions (e.g. no need to stop CPR for transfer or rescuer change)
- Less Injury to the patient during CPR
Potential Harms and Limitations
- Conflicting results have been seen in past studies of Mechanical CPR – some studies have shown worsening of mortality and neurological outcome
- Cost of Purchase and Cost-effectiveness
- Replaceable parts – a Zoll ‘life band’ costs in excess of $130
- Device Cost – an initial outlay on the equipment is required to provide mechanical CPR
- Training – staff need to be highly trained in the safe and effective use of the equipment
- Cleaning and Maintenance
- Time Taken to Place the machine effectively on the patient
Specific Mechanical Devices
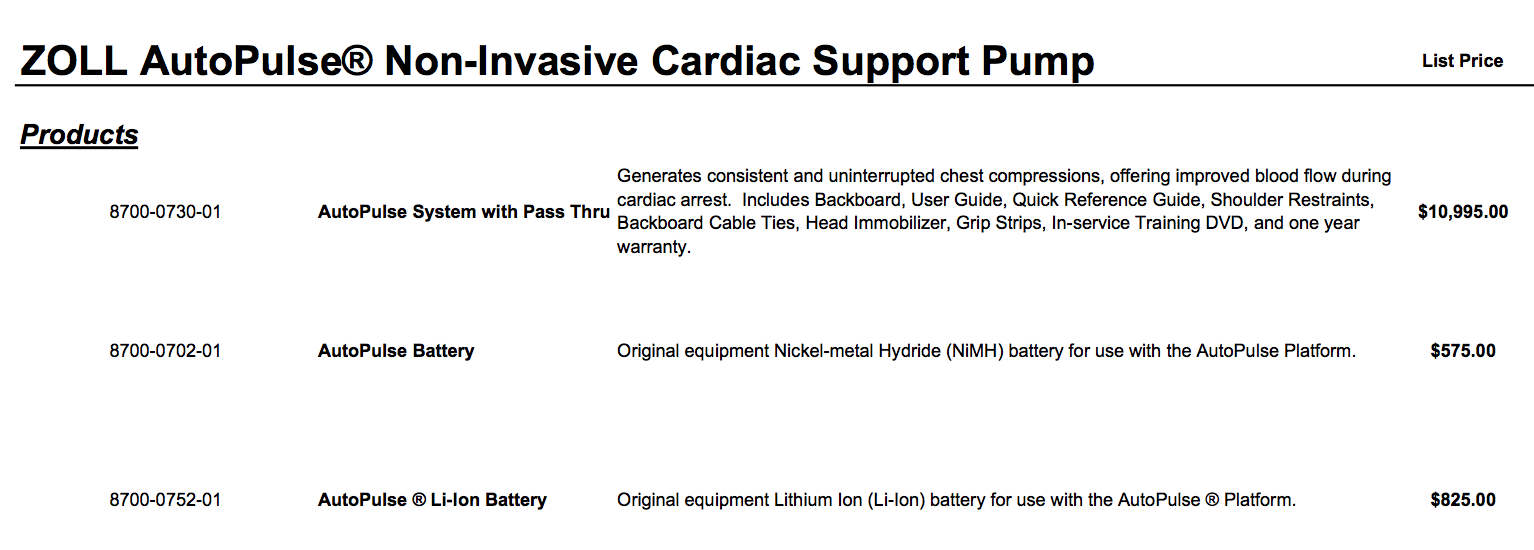
- Zoll

- Cost
- Zoll Limitations
- Only use in patients under 130kg
- Only use in patients over the age of 18
- Only use in ‘non traumatic’ cardiac arrest
- Pros
- Circumferential band is less traumatic than thumper or manual CPR
- Potential to read rhythm and give DC shocks ‘through’ on-going CPR
- Relatively Easy to put on
- Automated System
- Cons
- Cost (of both unit and disposable parts)
- Noisy (but less so than the pneumatic devices described below)
A Brief Video of the Zoll AutoPulse in Action
A Longer Tutorial Exploring Functions and Menu System
- Michigan Instruments
- Pneumatic Thumper Device

- Thumper Costs
- In the range of 1000 dollars (variable price)
- Limitations of the Thumper Device
- Overall Crudeness
- Portability
- Pros
- Familiarity (device has been available since the 1990s and was widely used in some centres)
- Cost
- Cons
- Trauma (rib/sternal injury)
- Can be difficult to attach to the patient
- Continues to ‘thump regardless’ – may injure patient or staff
- Noisy
- Physio Control
- Lund Hospital Cardiac Arrest System
- ‘The L.U.C.A.S. 2 Device’

- Costs
- The LUCAS 2 is in the range of $15,000 to $20,000
- LUCAS Limitations
- Only in adults
- Contraindicated in very obese or pregnant patients
- The Original LUCAS had a high pressured gas consumption and a theoretical fire risk when O2 was used as the pressurising gas
- Pros
- Creates an active ‘decompression suction’ on upstroke
- Portability (can be moved in bag and easily assemble)
- Can work off a mains power supply or battery source
- Cons
- Training – adjustment is not automated unlike the AutoPulse
- Trauma (rib/sternal injury)
- Battery needs to be in housing for device to work
- Cost
- Compressed gas consumption
- Noisy
- Initial Pilot Study of its use failed to show benefit
The LUCAS Device
Conclusions
Mechanical Cardiopulmonary Resuscitation is likely to have an increasing role in the future of CPR. Despite a lack of a current evidence base for its use it may be useful in selected cases especially where prolonged CPR is required. For example, it may be helpful to use Mechanical CPR in patients with refractory VF, Thrombolysis for Massive PE, Toxicological Arrest, Hypothermic Arrest and in arrested patients who are being transferred onto rescue VA ECMO.
Mechanical devices increase the efficiency and quality of CPR provided in experimental studies, which should intuitively improve outcomes. However, in a clinical setting further studies are needed to confirm or refute the benefit of these devices in real life practice.

New St Emlyn’s overview from Manchester following further recent studies – http://stemlynsblog.org/jc-paramedic-trial-m-cpr-st-emlyns/