
Vodcast
A Case to Consider
- A 42 year old male presents to the Emergency Department with Progressive SOB and Myalgias.
- He has a fever and tachycardia at triage.
- His initial BP is 90/60. He is treated with broad spectrum antibiotics and 3.5L of crystalloid IV Fluid

- On day 2 of admission Chest X-ray shows progressive lung infiltrates with a normal heart size. He requires intubation with mechanical ventilation and is transferred to the Intensive Care Unit

- Arterial Blood Gas shows PaO2 of 50 mmHg (50% Oxygen)

What are your differentials for the X-ray shown above?
- ARDS
- LVF / ‘Fluid Overload’
- Lymphangitis Carcinomatosis
- Pulmonary Haemorrhage
- Interstitial Lung Disease
- Valvular Heart Disease
- Other rare causes of bilateral infiltrate (TRALI, fungal, pneumonitis)
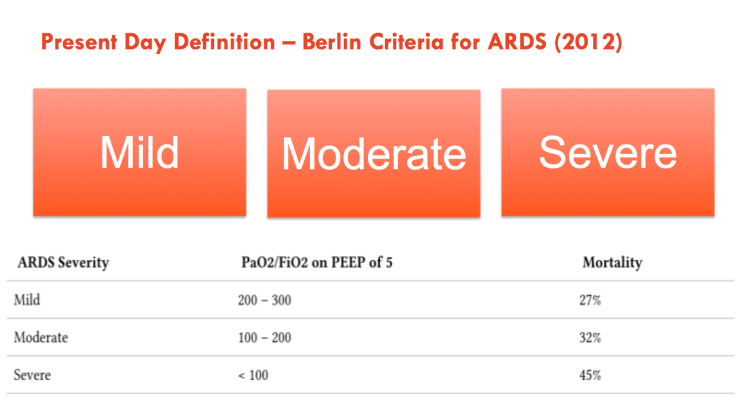
What are the current diagnostic criteria for ARDS?
- ARDS is a clinical diagnosis. Mortality is high (20-50%)
- Typical Features include:
- Acute onset
- Diffuse bilateral CXR changes**
- Varying degrees of relative hypoxaemia (ranging from mild to severe)
- Underlying cause – either ‘direct‘ or ‘indirect‘ injury
**Absence of Congestive Heart Failure (CHF) or Left Atrial Hypertension (Historically Pulmonary Artery Capillary Wedge Pressure was a diagnostic criteria. This has been removed because CHF can co-exist with ARDS )
What are the common causes of ARDS?

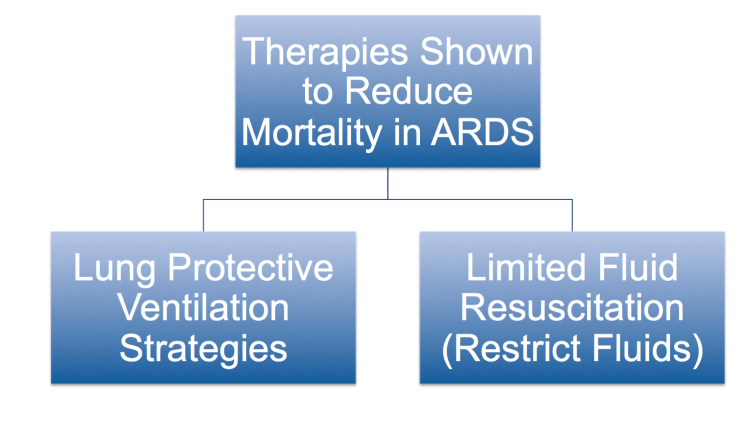
What are the potential treatments?
Cure starts with prevention… In the ED always use a lung protective ventilation strategy in the ventilated critical care patient.
Many of the treatments for ARDS are non-specific. Good intensive care is the mainstay of treatment. This includes a full package of high quality supportive care (FASTHUG).
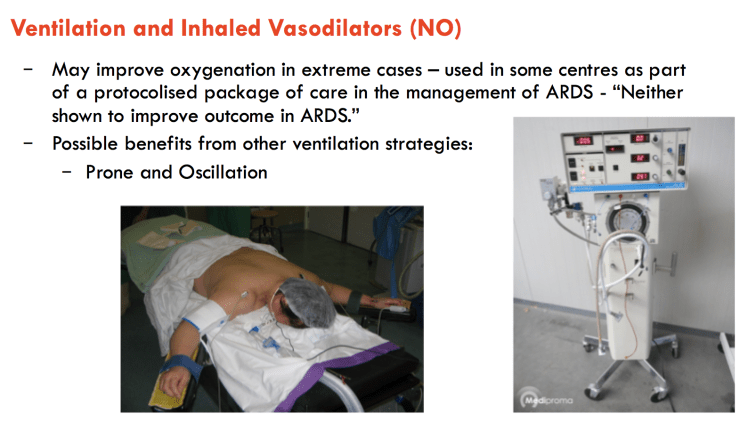
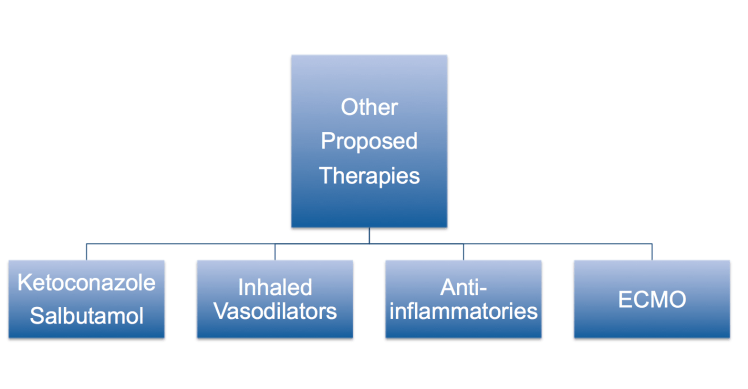
Ventilation (low volume) +/- prone positioning and Limited Fluids appear to be mainstays of treatment in ARDS. Vasodilators do improve oxygenation in severe cases but have not been shown to improve survival. Extracorporeal Membrane Oxygenation (ECMO) is a rescue therapy for refractory cases. Other promising therapies have been placed on the scrapheap for now including ‘antifungals‘, ‘beta agnoists‘ and ‘anti inflammatories‘
Summary – ARDS treatment should be focused on prevention, ventilation strategies and treating underlying cause. Good critical care principles are paramount.
ARDS FOAM resources
- ARDS – SMACC Gold
- ARDS Ventilation – Deranged Physiology
- References – Critical Care Reviews
- LITFL – Review
- CanadiEM – Review

http://lifeinthefastlane.com/ccc/prone-position-and-mechanical-ventilation/
Logistics – http://emcrit.org/podcasts/logistics-proning/