
A Clinical Scenario
A 70-year-old woman presents to the Emergency Department (ED) with an episode of collapse at the supermarket.
A bystander calls an ambulance and by the arrival of paramedics a few mins later the patient is lucid and responsive. She is found to be Hypotensive (91/50), Febrile (38.9 degrees), Tachycardic (105) and has an increased Respiratory Rate (>25).
On arrival in the ED she is seen quickly by the medical team and started on the local “Sepsis Pathway”. She states that she has recently been diagnosed with Liver Cirrhosis and Atrial Fibrillation. On a recent admission her Albumin Level was low and associated with deranged Liver Function Tests (LFTs).
On examination she is found to have bilateral swelling of both lower limbs with associated asymmetrical cellulitis (worse in the left leg). Having been diagnosed with Sepsis associated with the cellulitis she is started on appropriate broad spectrum antibiotics.
The Albumin level today is 17 (Reference Range 35-50 g/L) and the patient remains hypotensive after a 20ml/kg crystalloid bolus. The patient was given 4 units of Albumin over a 3 hours with some evidence of improvement in their haemodynamics.
This case scenario raised a number of questions regarding fluid resuscitation and hypoalbuminaemia:
-
What is albumin?
-
What is the association with a low serum albumin and Mortality?
-
What are the causes of a low albumin (Hypoalbuminaemia)?
-
Should we replace albumin in critically unwell patients and/or in the ED setting?
-
What are the Pros and Cons of giving Albumin?
-
What is the evidence for administration of Human Albumin?

What is albumin?
- Albumin = a water-soluble, globular serum protein of molecular weight 65,000
- Albumin = a ‘Colloid’
- A Colloid fluid refers to substances of large molecular weight (e.g. >30,000) in a solution.
- In humans plasma proteins are the main colloid
- In normal physiological conditions the liver produces around 200 mg/kg per day of albumin
- Albumin = 80% of normal plasma colloid oncotic pressure
- Albumin = 50% of protein content
- Albumin = a weak acid
- Albumin = is a major unmeasured anion and contributes much of the value of the anion gap. Every ’10’ decrease in albumin the anion gap (AIG) will go down by about 2.5
- For every 10 below the Normal Albumin add 2.5 to the Anion Gap
- *Normal Albumin is 40g/L so for an Albumin of 30 add 2.5 to AIG
- Albumin = has a half-life in plasma of around 20 days (an infusion will be redistributed after about 1 week)
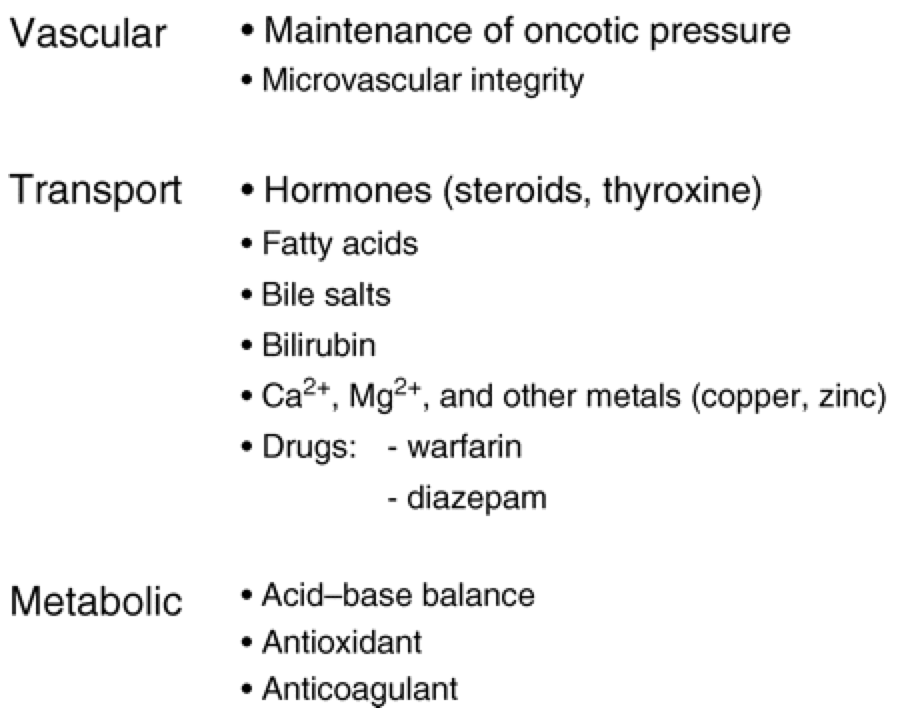
- Albumin = has multiple important physiological functions
The functions of albumin are summarised as follows (adapted from Boldt 2010)

What is the association with a low serum albumin and Mortality?
- Albumin is associated with an increased mortality in many prospective cohort studies and has been shown to be as good as the APACHE II and SAP II scores in predicting outcome in Surgical, Burns and Trauma patients.

- Low albumin may be an independent predictor in the Emergency Department for Trauma patients
What are the causes of a low albumin (Hypoalbuminaemia)?
- (1) Reduced Synthesis of Albumin
- Liver Disease
- Acute Phase Response (increased vascular permeability due to sepsis, trauma or surgery)
- Malnutrition
- Malabsorption
- Malignancy
- (2) Increased Loss of Albumin
- Nephrotic Syndrome
- Enteropathy (protein-losing)
- Burns
- (3) Haemodilution
- Pregnancy
- Postural
- Pseudohypoalbuminaemia (drip arm)
Should we replace albumin in Emergency Department patients?
The patient described above would seem a reasonable patient to replace albumin for in the first instance. She has significant liver disease and now presents with septic shock. However, she has no ascites and spontaneous bacterial peritonitis (SBP) seems less likely. We discuss the overall paucity of evidence for albumin in Critical Care below. Given its cost, many have concluded that it should be restricted to highly specific indications. In the Emergency Department these may include the following:
- Liver disease (associated with renal dysfunction)
- Drainage of Ascites (with significant volume)
- SBP
- Sepsis (in specific circumstances)
The use of albumin in burns patients, trauma, surgical and other medical patients may be best limited to judicious use in the Intensive Care Unit or Ward setting.

What albumin is available for administration to patients?
- Preparations of Human Albumin are widely available in heat-treated form
- In Australia they are manufactured by CSL and made from pooled human plasma
- They undergo alcoholic precipitation and pasteurisation for at least 10 hours at >60°C

- Various Concentrations are available diluted in normal saline
- 4%, 4.5%or 5% solution (50 g/L) (‘salt rich’)
- 20% solution (200 g/L) (‘salt poor’) – given in small volumes (20% is slightly hypo-osmotic and very hyperoncotic)
- 20% albumin solution has a very high Colloid Osmotic Pressure and can expand the plasma volume by 4 times the volume infused. Plasma volume expansion occurs at the expense of the interstitial fluid volume. A basic schematic illustration of this process is outlined below.
Simplified Fluid Compartment Model (in a 70kg man)

Infusion of 4.5% Albumin

Effects of Infusion = Expansion of Plasma Volume

What are the Pros and Cons of giving Albumin?
Pros
- May be useful in specific situations to expand plasma volume
- Possible marginal benefit in severe sepsis – See Critical Care Review
- Theoretical benefits – oxygen radical scavenging and plasma protein binding of toxins but no proof of benefit in clinical setting
- Anecdotally favoured by many critical care practitioners despite a paucity of evidence to suggest benefit
- Acute Respiratory Distress Syndrome (ARDS) patients in the SAFE study did better with albumin
- ARDS patients had improved haemodynamics when given diuretics and albumin in a 2005 study
- Overall, albumin is associated with improved outcomes in patients with severe liver disease
- In a low albumin state associated with liver disease Albumin may reduce mortality
- In a low albumin state associated with liver disease Albumin may reduce renal failure
- May improve response to diuretics in liver patients
- May prevent the ‘Post Paracentesis Syndrome‘ after an ascitic tap (i.e. deleterious changes to circulation associated with a risk of renal dysfunction, haemodynamic instability, rapidly recurrent ascites and dilution hyponatraemia)
Cons
- Human albumin solutions are more expensive than other colloids and crystalloids
- Viral Transmission (minimal risk of viral transmission because albumin preparations are heat-treated)
- Allergic reactions (rare),
- Coagulopathy (rare) – mostly due to dilution
- Limited evidence base of advantage over crystalloids – The Cochrane Review concluded:
“For patients with hypovolaemia, there is no evidence that albumin reduces mortality when compared with cheaper alternatives such as saline. There is no evidence that albumin reduces mortality in critically ill patients with burns and hypoalbuminaemia.“
- Increased mortality in Trauma patients
- Contamination has been reported as an issue
What is the evidence of the administration of Human Albumin?
SAFE Study (Finfer et al)

- No overall benefit in primary outcome of 28 day mortality from 4% albumin in ICU patients
- Almost 7000 patients
- Patients with Head Injury did worse in later analysis
- This may be because the fluid is hypo-osmolar
- SAFE Study Commentary as a varied interpretation
Cochrane Review (Roberts et al)
Looked at the effect of giving albumin compared with saline in critically ill or injured people and concluded that there was very limited evidence and that cost should significantly limit its use.
Critical Care Review (Myburgh et al)
Conclusions – “Although the SAFE study confirmed the safety of using albumin compared with saline in a heterogeneous population of critically ill patients, and many ICU clinicians con- tinue to favour colloid resuscitation, there is no definitive evidence that colloid solutions offer benefits over crystalloid solutions such as saline. Crystalloid solutions appear equally effective and are substantially cheaper; use of saline is associated with significantly improved outcomes in patients with traumatic brain injury. The use of colloids in patients with severe sepsis requires further study to determine firstly whether starch is safe, and secondly whether the use of any colloid improves outcomes compared with crystalloid.”
Albumin Indications Overview (Liumbruno et al)
FOAM – Fluid Resus Overview
FOAM – Albumin Overview
