Update on Mechanical CPR – 2014
- Dr Anantharaman (from Singapore) shared his expertise about Mechanical CPR at the ICEM 2014 Conference in Hong Kong and I was an interested listener having recently posted on this subject.

Hong Kong – ICEM 2014

- There is a need for improving CPR quality in all countries as survival rates are poor
- In Singapore it can take >15 mins for trained rescuers to arrive at the scene of a Cardiac Arrest
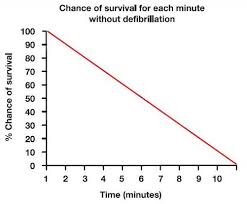
- Survival of CPR falls rapidly from the onset of arrest (see graphs below)
- Mechanical CPR may improve the quality of CPR (the second link in the so-called chain of survival)

- Emergency Medical Systems (EMS) face challenges for transport – both in terms of safety and in terms of the quality of CPR provided in transport – mechanical CPR may help in this respect

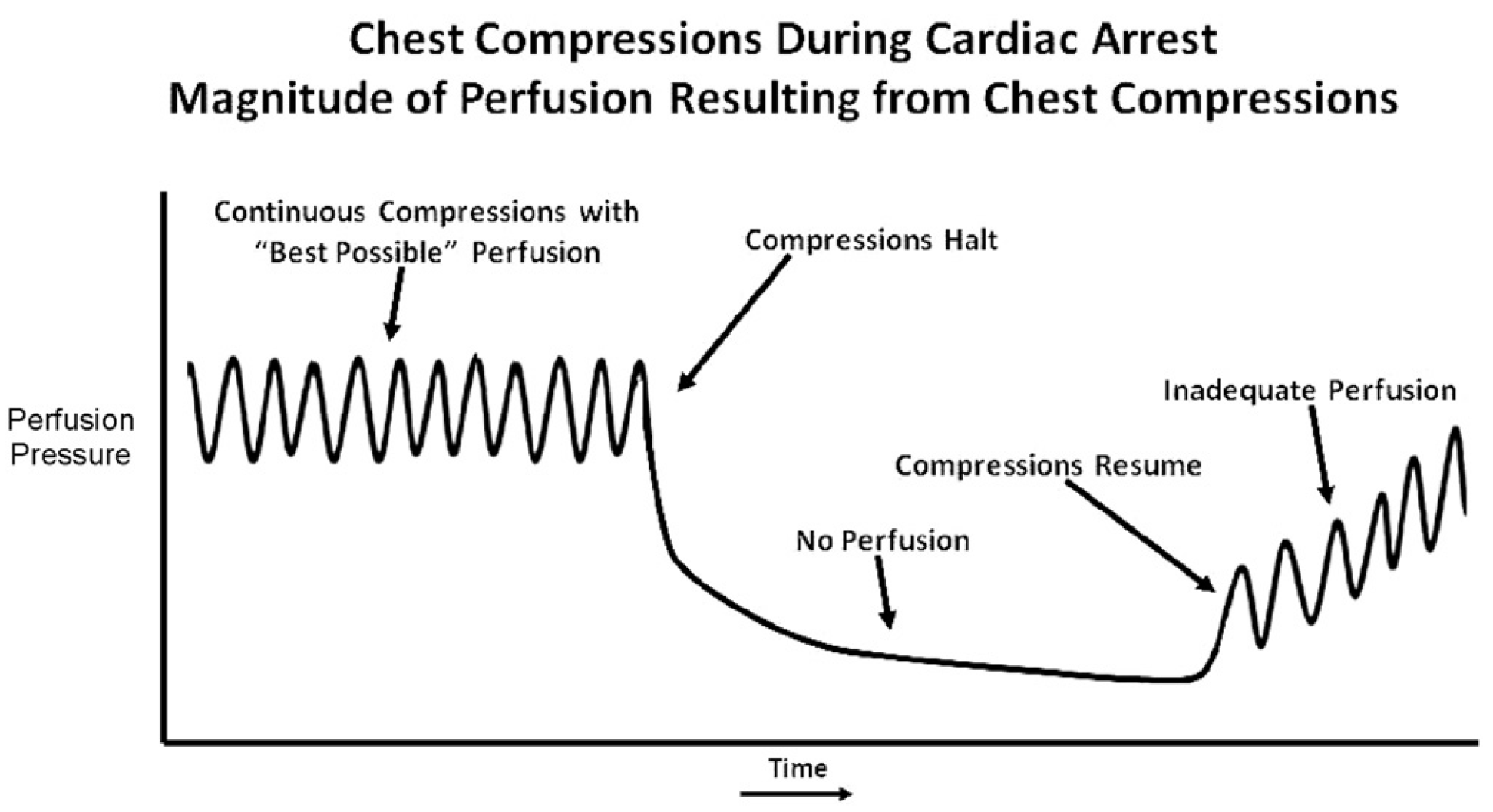
- Minimal Interruptions to CPR is ideal because it takes multiple compressions to build up a pressure head:
- Background of Mechanical CPR
- Originally perfumed on Dogs (successfully) around 50 years ago
- Later Piston systems showed no mortality benefit in humans (but some haemodynamic benefit)
- Data to date has been mixed on modern devices such as the LUCAS and AUTOPULSE
- One notable 2006 JAMA paper suggested potential HARM from mechanical CPR:

- More recent studies have suggested no benefit from the current devices but with some methodological issues
- The Speakers atICEM suggest that further studies are required due to these issues
- Clear rules on application of the Mechanical CPR and lack of standardised algorithms
- Use of intention to treat analysis – may affect results

- Recent Evidence on the various devices includes the following:
- AUTOPULSE Device
- CIRC Trial
- Survival in patients receiving Mechanical CPR has NOT shown benefit in recent trials such as the CIRC Trial (2011).
- However, the manual CPR in these studies was of higher quality than one would expect.
- The fraction of effective chest compressions was about the same between groups.
- CIRC Trial
- LUCAS Device
- LINC Trial
- 4-hour survival rate: Mechanical compression group (23.6%) versus the conventional group (23.7%)
- 6-month survival rate: Mechanical group (8.5%) versus conventional group (8.1%)
- 6-month good neurologic status (based on Cerebral Performance category of 1 or 2): Mechanical group (99%) versus conventional group (94%)
- MECCA Trial (Singapore)
- Provisional results of this as yet unpublished trial were presented:
- 1189 eligible patients
- Low levels of survival overall
- Higher survival in Mechanical CPR group but not statistically significant
- Provisional results of this as yet unpublished trial were presented:
- LINC Trial
- Using a “Pit Crew” method (Ong 2012) for implementing Mechanical CPR may reduce the time it takes to fit the device and maximised the time of chest compressions
- AUTOPULSE Device
Take Homes
- How do we deliver better chest compressions?
- Recent reviews of the evidence have suggested that is unclear whether Mechanical CPR has benefit
- The presenters at ICEM believe that Mechanical CPR may have a role – especially in transporting patients
- Modern devices may cause less injury compared to older Piston Types
- Good CPR requires Teamwork and Training regardless of whether human CPR or machine CPR is used
- Public Education on the importance of early CPR will save lives as Cardiac Arrest is a pre-hospital event with survival likelihood determined by early intervention (CPR and Defibrillation)
- AEDs which are now widely used in public buildings. In the same way technology such as Mechanical CPR devices may become increasingly available in the pre hospital setting.
- Mechanical CPR may have a future role despite the disappointing trial data described above
- Technology is likely to advance and more trials of implementation are required in this area
Further Listening – Lecture by Marcus Ong (2011)

New St Emlyn’s overview from Manchester following further recent studies – http://stemlynsblog.org/jc-paramedic-trial-m-cpr-st-emlyns/