

Introduction
There has been a bit of discussion where we work about the ECG questions on the recent Australasian College of Emergency Medicine Fellowship Exam.
While we initially only had a fleeting look at the ECG questions whilst on the way to a Lynyrd Skynyrd concert (i.e. setting a clear priority for study) the initial reaction was one of “what the”!
Indeed the first of two ECGs that we discuss here would certainly need more thought and deliberation than the 10 minutes normally allowed to write an answer for this type of question in the FACEM examination.

According to formal reports and candidate anecdote answers included ‘VT’, ‘TCA overdose’ and ‘some-kind of pacemaker malfunction’. Now that we have got our hands on the original examination paper, I thought we could take a longer look at the ECG question and then get the opinion of a true ECG expert – namely the legendary Professor Ken Grauer.

ECG Question 1

- Quite a tough question – leads to a number of initial reactions (described above) as well as a distinct visceral feeling…
- Of course, when answering these type of questions it is always important to Describe AND Interpret the ECG in the CLINICAL CONTEXT of the patient described in the case…
- From a Clinical point of view this patient is:
- Young
- Presenting with significant Cardiac Symptoms
- Hypotensive
- Presenting Acutely to the Emergency Department
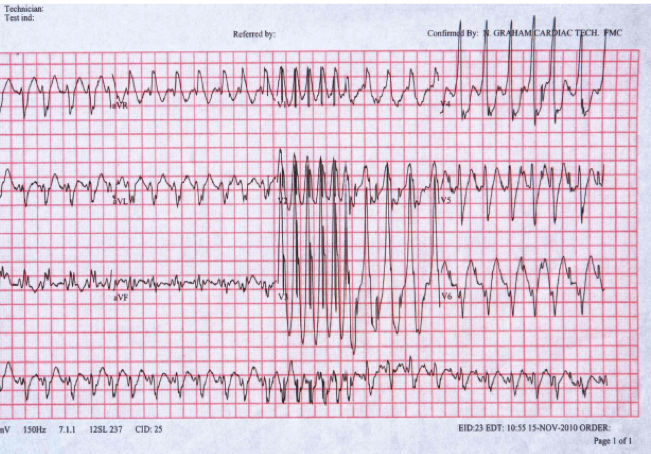
- At first glance this ECG is:
- A Broad Complex (very fast) Irregular Tachycardia
- Highly Abnormal
- Has a “WTF” appearance

In our travels we found Mel Herbert’s differential list for a ‘WTF’ ECG and this may be helpful in this case:
- Electrolyte abnormalities
- especially high potassium
- Toxicology
- Myocardial Ischaemia
- Wolf-Parkinson White (WPW)
- Lead misplacement or Artefact
- Pacemaker malfunction
We have discussed some of these on the ECG PAGE and FELLOWSHIP EXAMINATION PAGE
What about this ECG?
- This ECG is wide, irregular and very fast – approaching 300 in places.
- From our perspective a rate of 300 is highly abnormal and should be seen as a ‘red flag’.
- This rate is too fast for the normal conduction system of the heart
- So there must be an accessory pathway!
- The irregularity seen on the ECG (confirmed using a ‘card’ method) is most likely due to Atrial Fibrillation (AF) – so the best interpretation of this ECG is WPW with rapid AF.
Happily, Prof Grauer agrees with this answer:
He has an excellent blog post on this “cannot miss” ECG
What are the Implications of this uncommon ECG finding?
- The patient is unstable
- This is a Time Dependent Cardiac Emergency
- The patient needs Urgent Cardioversion
- Chemical cardioversion has potentially catastrophic consequences and therefore electrical cardioversion is preferred with judicous analgesia/sedation
Does the abnormal R wave suggestive of Sodium Channel Blocking Drug Toxicity?
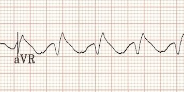
A dominant R wave in AVR (associated with TCA Overdose), Right Bundle Branch Block and WPW with AF seem to all look very similar. Looking closely at AVR in THIS CASE it seems that in this case the S wave is in fact very prominent and it is hard to define the ratio between R wave and S wave. Commenting on the abnormal appearance of AVR and lead V1 in this case and a possible differential is reasonable and recommended.
Further Discussions on AVR “the often forgotten lead” can be found HERE and HERE
Prof Grauer kindly has donated a section of his e-book on AVR – The ECG and Lead aVR
AVR IN THIS CASE

Comparative Examples of Dominant (or “terminal”) R waves in AVR


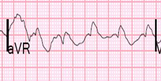
Various Appearances of AVR seen in Right Bundle Branch Block
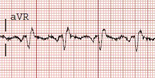

What are the cause of a Dominant R Wave in AVR?
- Sodium Channel Blockade (Na Blocker Toxicity)
- Lead Misplacement
- Dextrocardia
- Atypical RBBB
What are the cause of a Dominant R Wave in V1?
- This finding is seen in less than 1% of ED patients and has a broad differential
- RVH – Normal Paediatric ECG or Pathological Right Ventricular Hypertrophy
- Right Bundle Branch Block
- Myocardial Infarction (Posterior)
- WPW Syndrome
- Incorrect lead placement and Dextrocardia
- Cardiomyopathy and Muscular Dystrophy
- Diastolic Overload
Conclusion / Take Home
So, fast, wide, irregular and weird looking: think WPW with Rapid Atrial Fibrillation (or if you’re South African or English, think of the cricketer Mitchell Johnson as a way of remembering this)

ECG Question 2
The second question has been equally divisive.
Exam candidates are frequently told that in a Visual Aid Question (VAQ), every word in the stem is important. Indeed, when the examiners tell you a patient’s weight and BMI in an ECG question, they are giving you a huge clue!
So what is YOUR interpretation of this ECG?
When you are told the patient is very underweight this is likely to be a contributory factor if the examiners have taken the time to tell you. Possibilities (before you even look at the ECG itself) would include electrolyte problems, drug use, toxins, cardiomyopathy, heart blocks and hypothermia.
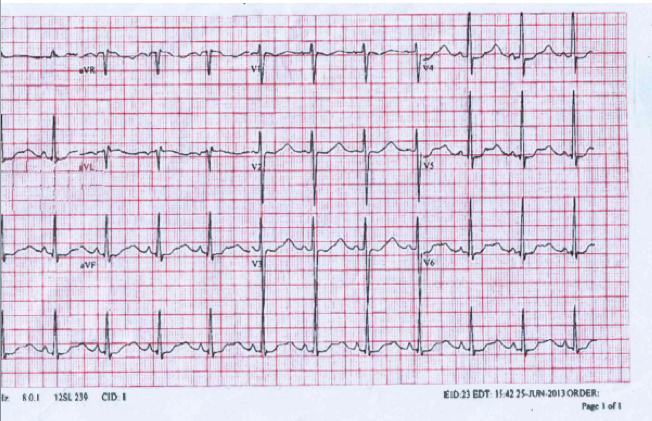
Here’s Prof Grauer’s interpretation
“Question 8 – I see sinus rhythm – and normal PR and QRS intervals – but a long QT. This most likely is really a long “QU” interval – as several leads appear to show a double peak. When the U wave becomes very tall – it often fuses with the T wave, making distinction between the 2 waves difficult. Otherwise – there is diffuse ST flattening and depression. Given the above history and this ECG – I would be strongly suspicious of marked hypokalemia (and marked hypomagnesemia). I suspect this very slender 15yo girl has bulimia – so more history, checking mouth, talking to family, etc for more diagnosis of this potentially life-threatening condition if she doesn’t get treatment. I would NOT send this 15yo girl home!”
For more on this – Click Here
Other Hypokalaemia ECGs – Case 15 on our ECG page
Further thoughts on this ECG
- In general – the ECG isn’t specific for hypokalemia. That said – when the “setting is right” (as it is here) and especially when the U wave is present and taller than the T wave (as it is here) – the diagnosis is much more likely.
- While diffuse ST depression could be ischaemic in origin if the clinical setting was different – it is hard to imagine anything but hypokalaemia for the setting given here.
- Often forgotten when serum K+ is low it becomes HIGHLY likely that the Magnesium is also low.
- Moreover – you often won’t be able effectively to correct serum K+ until you correct serum Mg++.
- Hypokalemia sometimes (for unknown reasons) produces a “pseudo-P-pulmonale” pattern. This is present here – as we can see, while not overly tall, the P waves in II,III,aVF are much more pointed than is usually seen.
Conclusions
Emergency Doctors need to recognise the ‘common’ and the ‘commonly deadly’. Many cases in real life clinical practice that are important to diagnose will fall into the latter group. While we don’t want to invoke an “exam mentality”, if we were the examiners we’d want to be sure that Emergency Specialists knew about very rapid AF with WPW and about clear signs and context consistent with hypokalemia so these two questions while certainly challenging are fair (and have come up in the exam before in the past). From an “exam centric” point of view – try to get in the examiners head – Question 1 if more likely to be AF with WPW rather than TCA given the history given and very rapid rates.
Acknowledgements
Thanks again to the Ken Grauer, a true gentleman, who over the years has patiently answered many questions that we have sent him from Westmead. For those who aren’t familiar with his work we would thoroughly recommend both his book “ECG Pocket Brain 2014” of which Toby and Andrew are both proud owners.

Thanks for the kind words Andrew. Both of these are challenging but very important Board Questions – and highly rewarding in that astute ECG interpretation allows rapid recognition of what otherwise is a potential life-threatening situation for which appropriate treatment makes a difference.
Thanks ken. It’s great that the ACEM exam has such a strong focus on ECGs
There are some questions about the issue of AVR in ECG 1 – in terms of the question – the patient seems to have more Cardiac than “tox” symptoms and the ECG doesn’t have the classic “dominant R wave” in AVR consistent with a TCA Overdose. For any VAQ (as you would in real life) it is important to consider a Broad Differential. Once you have looked at the ECG and ‘described’ the findings the interpretation has 3 components – Conclusion(s), Differentials and Implications.
So for example in this case:
CONCLUSION – Broad Complex (very fast) Irregular Tachycardia
DIFFERENTIALS – WPW with AF, Toxins (Na Channel Blockade), BBB with AF, Torsades
IMPLICATIONS – Time Dependent Cardiac Emergency – patient requires emergent Cardioversion in a monitored setting with judicious analgesia and supportive care