
- On the 21st of May 2014 The Emergency Medicine Interest Group (EMIG) had its annual “Not So Grand Rounds” session at Westmead Hospital.
- This was a well attended event due to the presence of great speakers (as well as the attraction of free Pizza).
- A case vignette (discussed below) was presented as part of Not So Grand Rounds.

The Case Vignette
Setting the scene
You are working on a busy shift in the Emergency Department (ED) – a young patient has been admitted with a respiratory infection. He is in the Short Stay Unit (SSU) and you are called to see him because of increasing Shortness of Breath and Chest Pain at 0200.
Briefly reviewing the notes you find the following history:
- The patient is male and 20 years old
- The previous day he had presented to the ED having been asked to attend by his General Practitioner (GP).
- On arrival in the ED at 10pm he was complaining of moderate Chest Pain.
- He described a sudden onset of chest pain at 3am (some 12 hours prior to arriving at triage)
- At triage his complaints included:
- On-going Shortness of Breath
- Left sided lateral chest and Scapular pain that woke him from sleep
- The pain was worse on inspiration and intermittently worsening – it is not affected by position
- The patient was recently well and has had no previous hospital admissions
- Although family members had recently had upper respiratory tract infections he had been well up until the onset of symptoms. He had no fevers and although he had a mild cough there was no haemoptysis.
- There was no history of trauma, travel, immobility or surgery
- There was no past medical history of DVT / PE
- There is no history of smoking
- There is no history of asthma
Initial assessment and management included:
- An initial x-ray had shown no evidence of Pneumothorax (the main concern of the referring GP)
- A temperature of 38 degrees as well as respiratory symptoms
- As there was no evidence of pneumothorax and the team considered him to be “low risk” for Myocardial Infarction and Pulmonary Embolism it was felt reasonable to make a diagnosis of an infective cause
- A clinical impression that the patient had a respiratory infection with significant symptoms
- He was treated with appropriate antimicrobial therapy promptly after arriving

While reviewing the notes the following observations are recorded by the nursing staff:
BP 110/70
HR 109
Saturations 96% on room air
Respiratory Rate 28
Temperature 37.9 degrees celsius

At this point the patient is still complaining of chest pain on the left side…
What are your differentials?

Differentials
- Respiratory
- Pneumothorax
- Pneumonia
- Pulmonary Embolism (PE)
- Cardiac
- Acute Coronary Syndromes (ACS)
- Pericarditis
- Aortic Dissection
- Abdominal
- Oesophageal Rupture (Boerhaave’s Syndrome)
- Pancreatitis
- Other Causes
- Trauma
- Rib Fractures
- Epidemic Myalgia
- Viral Infection
- Muscular Pain
- Herpes Zoster (Shingles)
- Somatoform Disorders
What is the most likely Diagnosis?
Given the sudden onset of symptoms in this case as well as the age of the patient Pneumothorax was thought to be the most likely diagnosis in the first instance. However, the Chest X-ray (shown below) did not show a Pneumothorax.
The subtle triangular shaped area of opacification seen on the lateral x-ray (at the lung base) was thought to have reflected a diagnosis of early Pneumonia and he was treated for this as a result…


What Happened Next?
- At this point our young patient becomes more tachycardic and dyspnoeic. He spikes a high temperature.
- After further review it seems likely that he dose have chest infection. However, we elect to consider Pulmonary Embolism (PE) as a possible diagnosis at this stage…
- A 12 lead ECG is recorded (he was continuing to be markedly Short of Breath while this was taken):
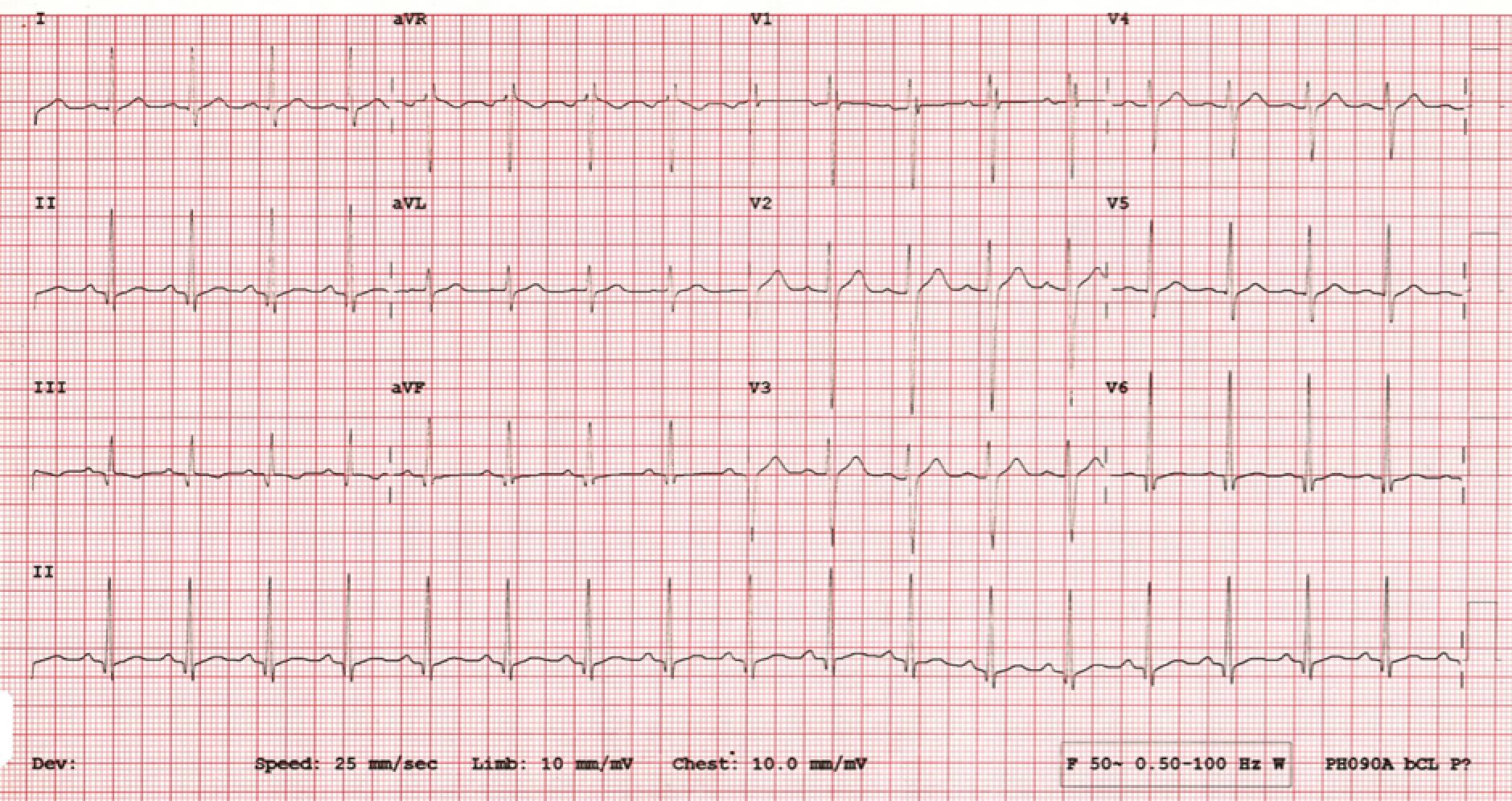
- The 12 lead ECG (shown above) showed a sinus tachycardia with right sided strain pattern
- In the meantime his x-ray (shown below) was repeated.
- His blood tests and blood gas were non-diagnostic and he continued to be symptomatic with breathlessness:

- The patient is appearing clinically worse despite antibiotics – his repeat X-ray (above) is concerning to the treating team. Could this be a pulmonary infarction associated with PE?
- After a period of consideration of the case it was decided to obtain a CT pulmonary angiogram
- This CT showed multiple bilateral pulmonary emboli
- The patient was treated with anticoagulation.
- 3 days later he was discharged home feeling much better with appropriate follow up.
How do we decide whether to investigate for a disease in the ED?
In this case the first treating clinicians had felt that the risk of PE was low.
What does this mean?
How do we decide what a patient’s risk for a given disease is?

The concept of risk is somewhat counter-intuitive. The individual patient either has the disease (100%) or he doesn’t (0%). However, we cannot do every test for every patient! Many patients have some (even if a negligible) risk of having a particular disease.
If we were to throughly investigate 100 health patients for Pulmonary Embolism we may find several individuals with evidence of asymptomatic (silent) PE. So should we screen and treat everyone for PE? The answer seems to be no if we want to avoid harm. We have no evidence that finding or treating a silent PE in a healthy patient is beneficial. In fact, ia workup for PE in a healthy patient may be harmful. Harm may be from the risk of investigations (CT scans) or from the risk of subsequent (potentially unnecessary) treatments such as anticoagulation.

The Test Threshold
Some clinicians use the Test Threshold to determine whether to investigate for a disease (typically we consider common and commonly deadly conditions as important to consider for further diagnostic work-up).
Click Here for more information on diagnostic workup
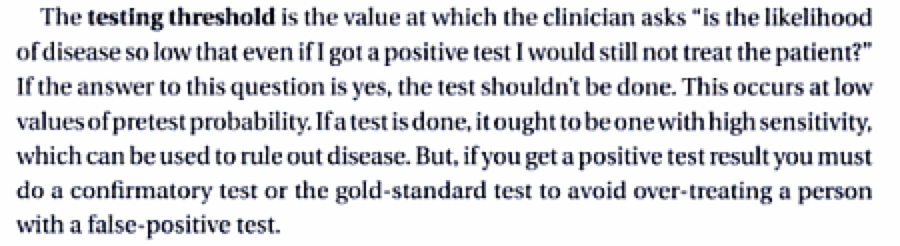
So, in summary, the Test Threshold is when the pre-test probability of the considered differential diagnosis (such as MI or PE) is very low. So much so that it is not worth pursuing the diagnosis in that patient because you will do more harm than good by investigating the patient. The “test threshold” is both mathematical formula and a bit of voodoo.
So if you think the patient has less than a 2% chance of having a PE we should pursue another diagnosis. In a very low risk patient we can have a false positive CTPA, bleeding from the treatment and radiation risk from the CT (illustrated above). This is not to mention the cost in the healthcare team and patient’s time as well as the health system’s money!
Risk of PE
So, how do we decide what the risk is for PE?

- Gestalt – the opinion of an experienced clinician has shown to an be accurate risk predictor for PE
- Well’s Score
- Full Score – Click Here
-
- A score of ‘0 or 1’ = pre-test probability of 1.3%
- Pulmonary Embolism Rule out Criteria (PERC)
- Full Score – Click Here
- I think he’s < 10%: use PERC
- I think he’s > 10%: investigate the patient with further clinical work up and investigations
PE Workup Summary

Alternative PE Workup – Click Here
Summary
Thinking about important causes of chest pain and using judicious investigations for their diagnosis is a cornerstone of good emergency care.
In this Case Vingette we illustrated some of the pitfalls in the diagnosis and workup of the patient with Chest Pain in the Emergency Department.
We considered the ‘test threshold’ and its implications for when to use invasive investigations.
While we must always consider PE, ACS and Aortic Dissection in the patient with chest pain, we must be careful not to cause later harm by use of inappropriate investigations.

Thank you for good pre-breakfast reading. I’d have added lung ultrasound for laterobasal pleural line abnormalities, and a look at aortic root and pericardium, prior to the CT. Still not rule-out tests unfortunately, but helpful when resources are sketchy.
Thanks for the feedback IpswichUSS! – Our Lung USS skills are not up there but we have confidence that point of care echo will have an increasing mainstream role…
Lung ultrasound is much easier than echo, it is training wheels stuff.
Agree that EFAST is becoming a widespread skill. Though lung USS is simple to learn at a ‘point of care’ level, many ED doctors have less confidence interpreting lung USS than say a FAST or AAA scan. Do you think the future will be teaching medical students these type of skills?
Already mandatory undergraduate training in USA, which is 10 years behind Europe. Australia is very slow on uptake due to our superb sonography service. Mind you, I don’t think we should expect everyone to grasp it equally. I would be happy if everyone could recognise a good quality scan and understand its limitations.
It looks like Sydney Uni are bringing in more USS in their new curriculum