
ECG Cases
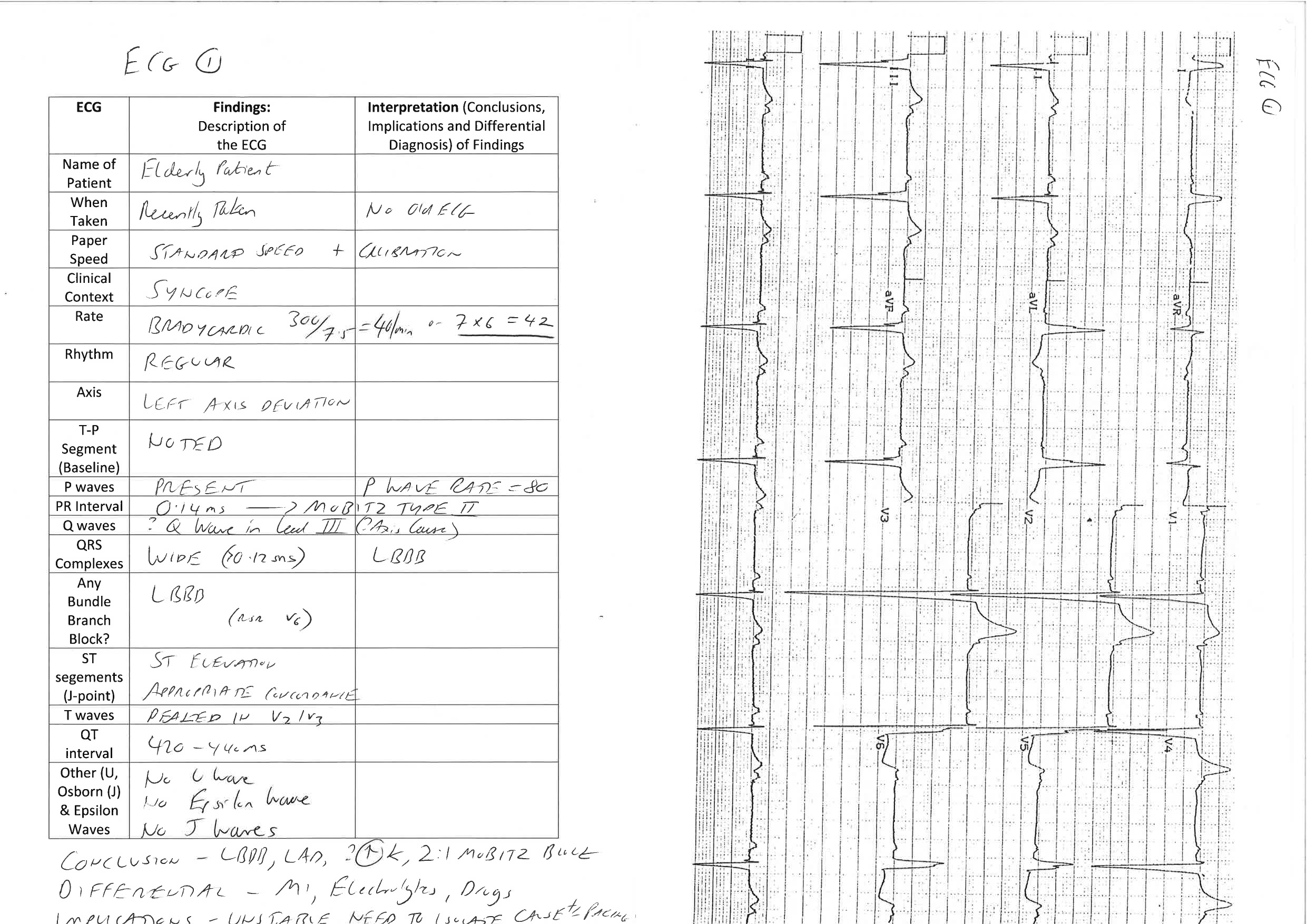
ECG 1 – A 60 year old male patient presenting with Syncope pre-dialysis:


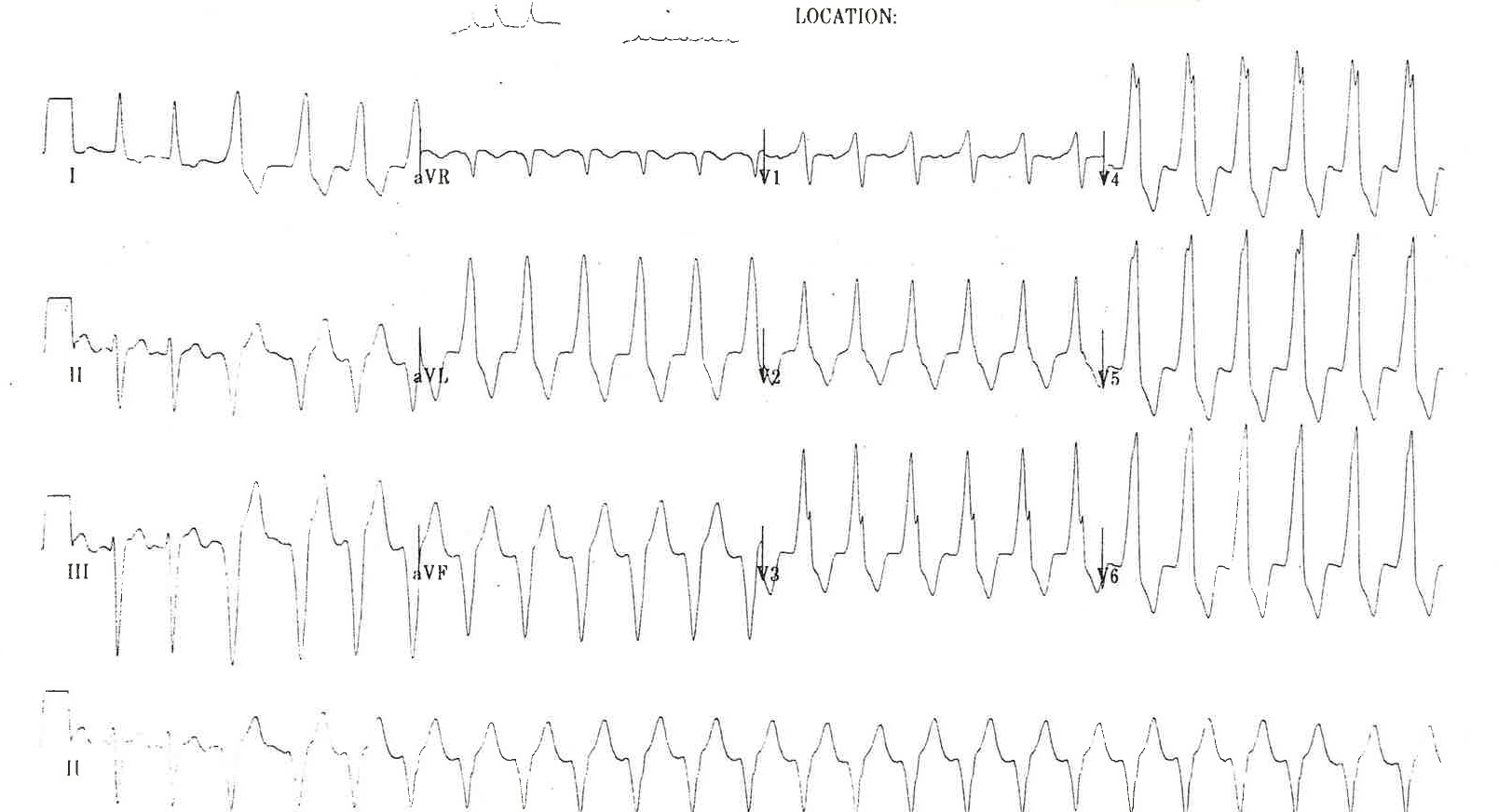
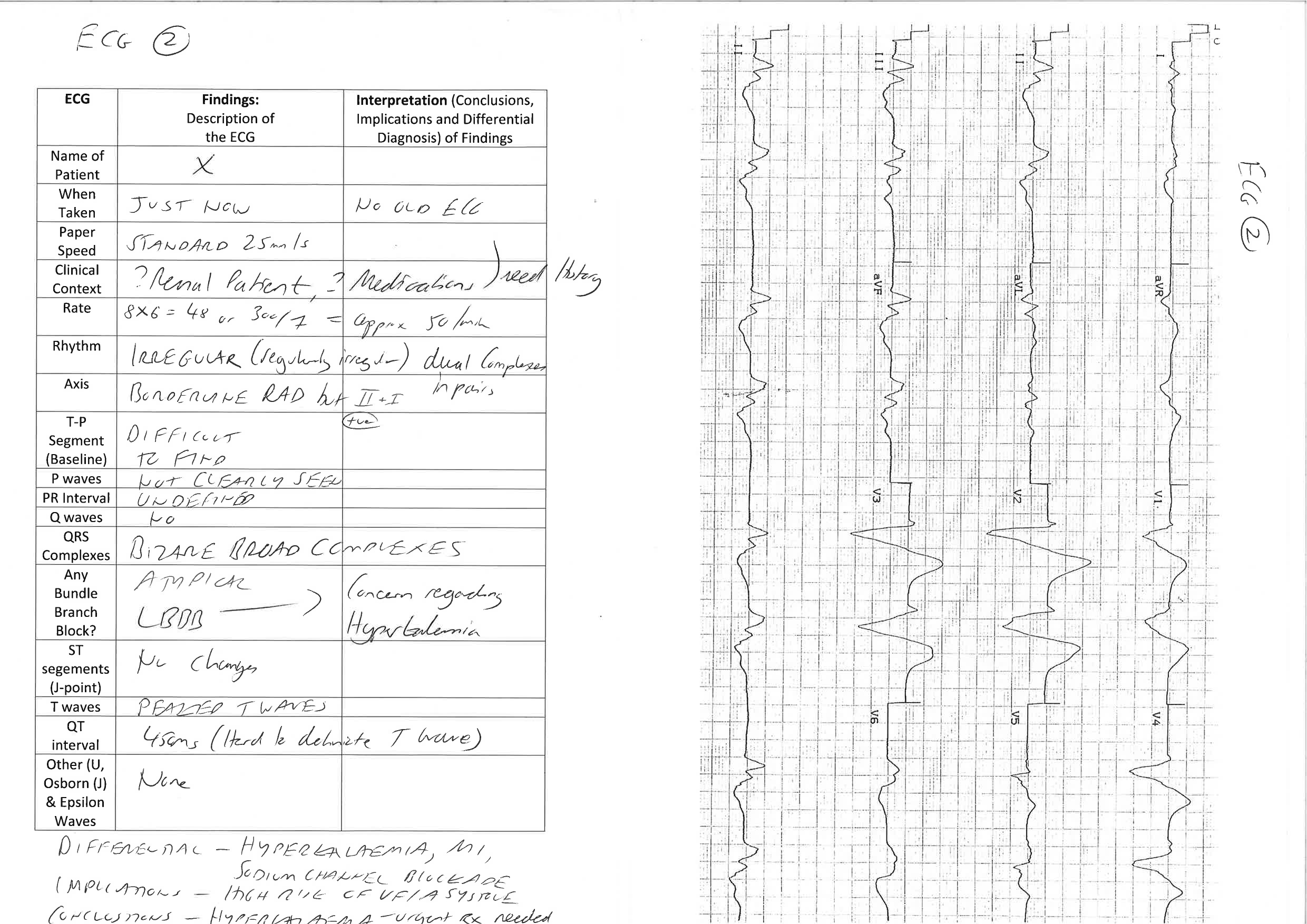
ECG 2 – A 30 year old female patient presenting with recurrent palpitations. Her heart rate is recorded at 190 on arrival:

ECG 3 – A middle aged smoker presents to the Emergency Department following a Cardiac Arrest – his ECG is taken on arrival following Return of Spontaneous Circulation (ROSC):
ECG 4 – An elderly man presents with light headedness and lethargy.
He is found to be bradycardic at triage with a blood pressure of 90/55:

ECG 5 – A man with a history of hypertension presents chest pain and palpitations. This is his 12 lead ECG:


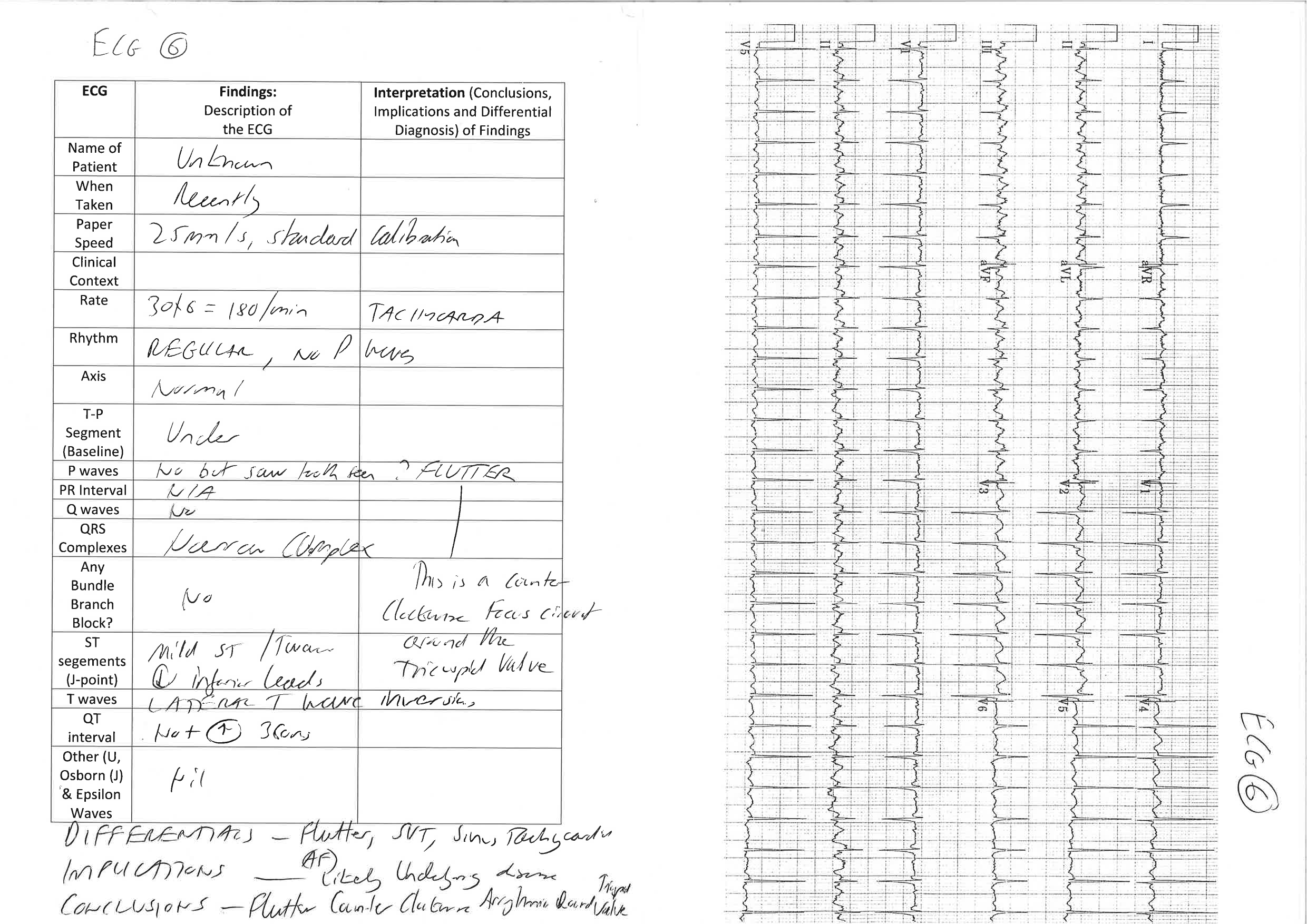
ECG 6 – a young male presents to the ED with flu like symptoms and a runny nose. He has a cough and mild chest pain associated with coughing paroxysms.
In the minors area of the ED the nursing staff perform a routine 12 lead ECG which is presented to you:
This ECG shows atrial to ventricular conduction via an accessory pathway (note the inverted P waves and very short PR interval with ‘delta’ waves). This ECG finding is highly suggestive of Wolf Parkinson White Syndrome (WPW), a relatively common condition affecting about 1 in 500 people. In WPW an accessory bundle (“bundle of kent”) can allow for conduction from atria to ventricle bypassing the normal AV node pathway. The resting ECG shows a short PR interval (<0.12 seconds), delta wave (i.e. slurred upstroke into the QRS complex) as well as broadening of the QRS complex. There are two main sub-types of WPW: Type A (+ve delta wave in V1) and Type B -(ve delta wave in V1).
Emergencies associated with WPW include arrhythmia (e.g. SVT and AF) as well as a small increased risk of sudden death. Treatment of acute rhythm disturbances is generally best achieved with DC cardioversion rather than chemical (medication) cardioversion. In WPW with associated Atrial Fibrillation (AF) there is a specific risk of precipitating malignant arrhythmia by using AV node blocking drugs such as Verapamil and Metoprolol because the AF is transmitted rapidly to the ventricles increasing the risk of VF. Follow up with a cardiologist sub-specialising in electrophysiology studies and radio frequency ablation is appropriate.
More on Wolf Parkinson White Syndrome in Emergency Medicine can be found at the following online tutorial:
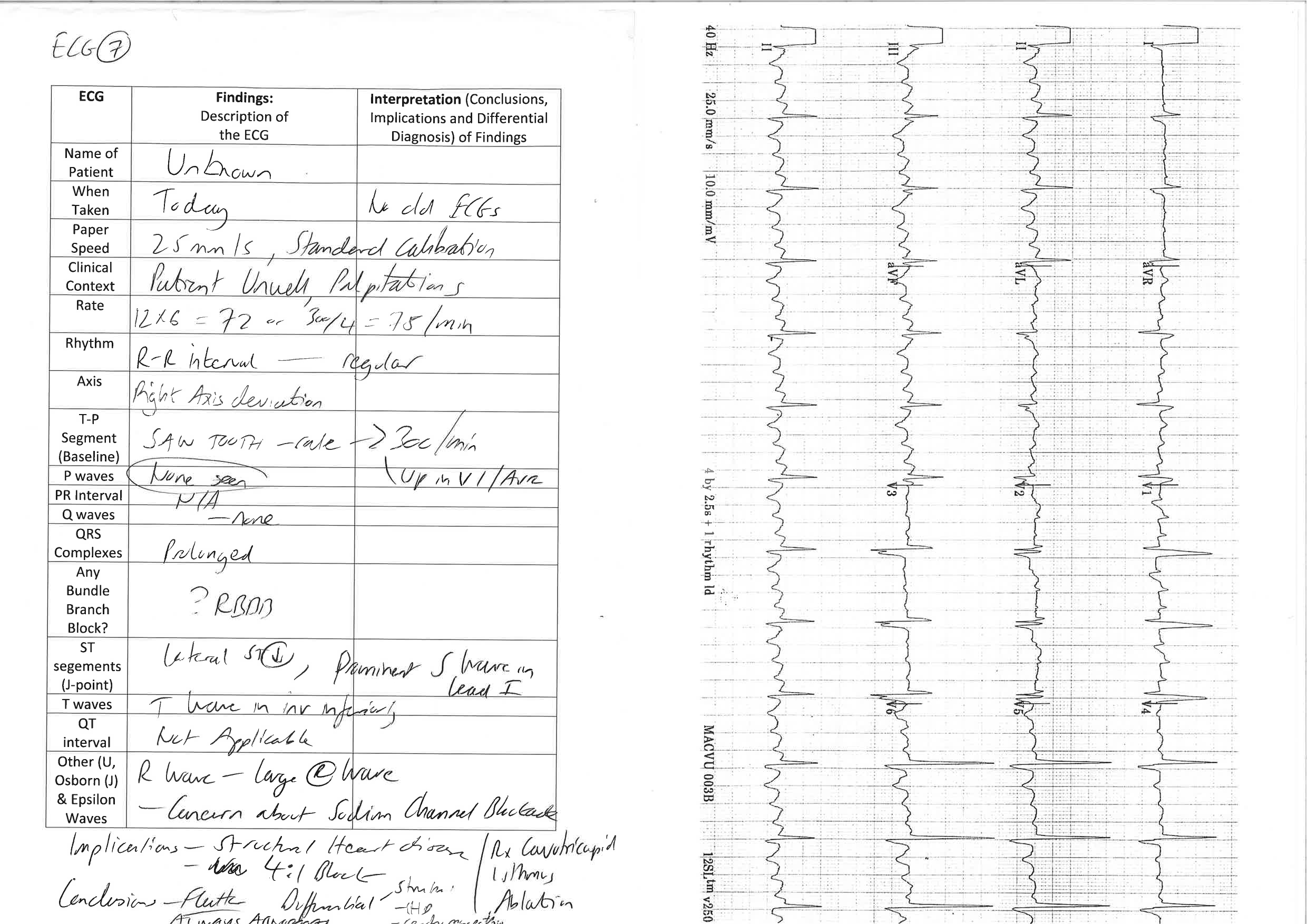
ECG 7 – Following a review by the local heart specialist a further ECG was taken showing a normal sinus rhythm and the patient was discharged home with outpatient follow up:
ECG 8 – A different patient presents with palpitations and a history of WPW:
ECG 9 – The patient from ECG Case 8 has a further ECG taken after resolution of his symptoms:
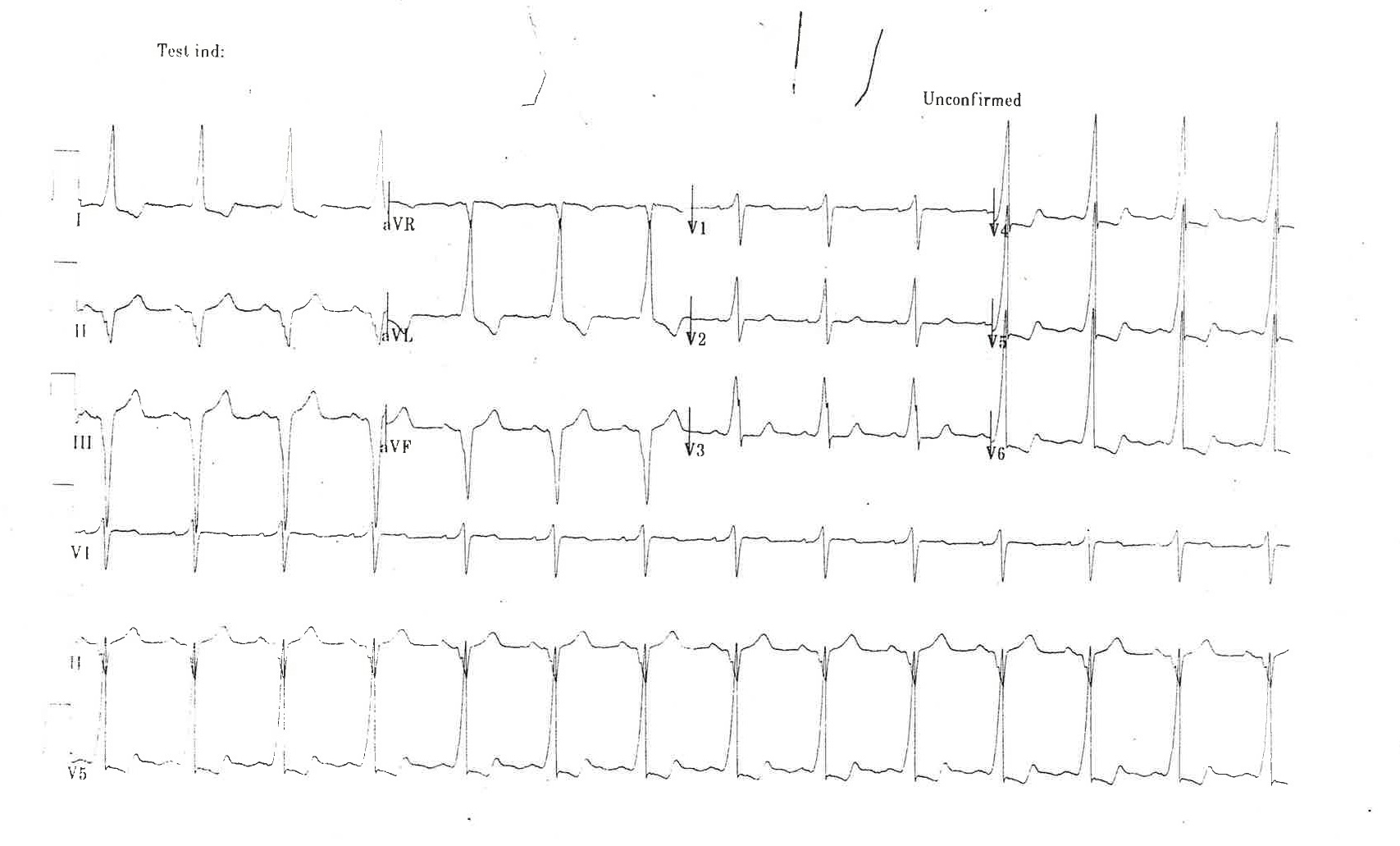
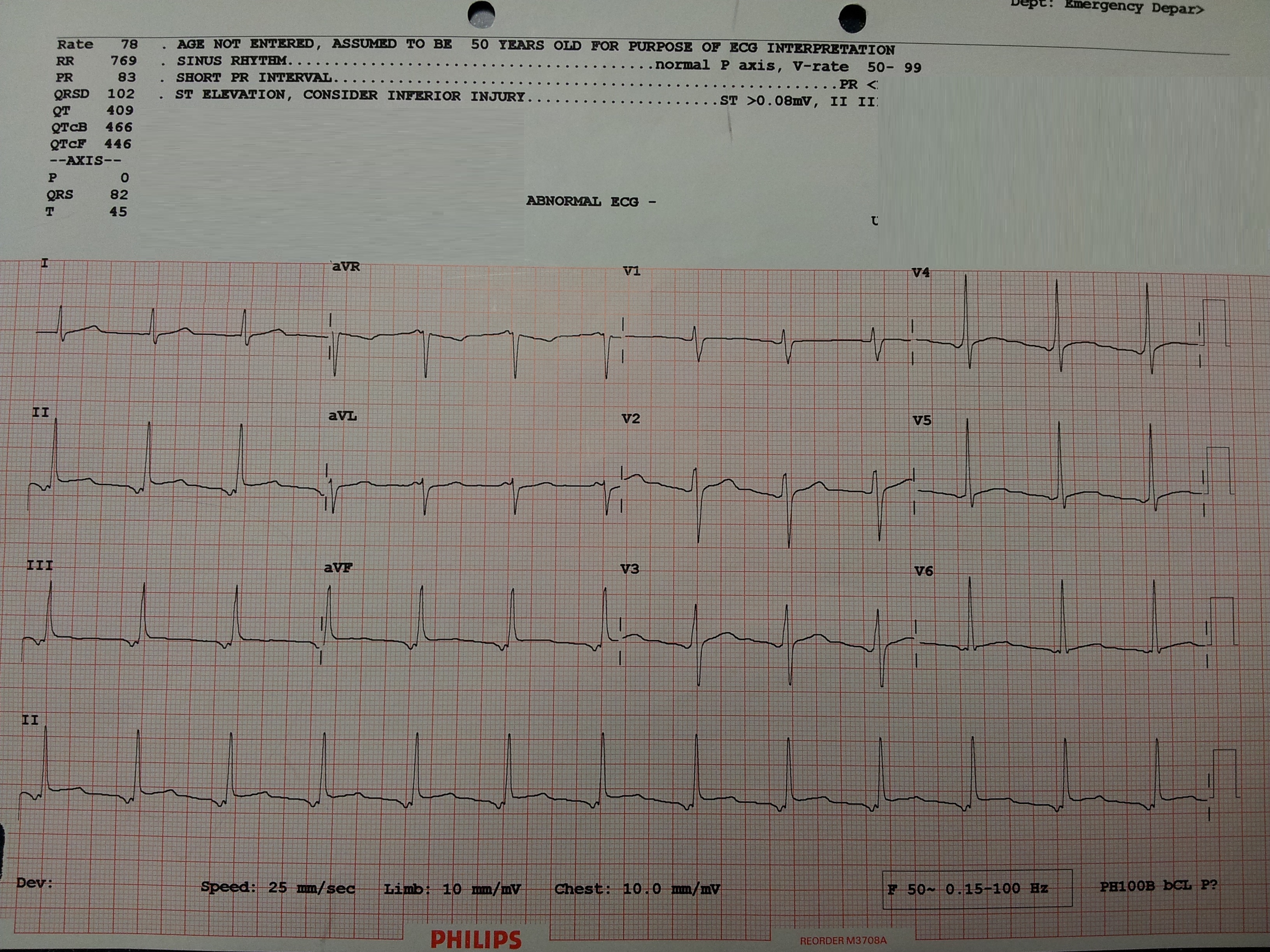
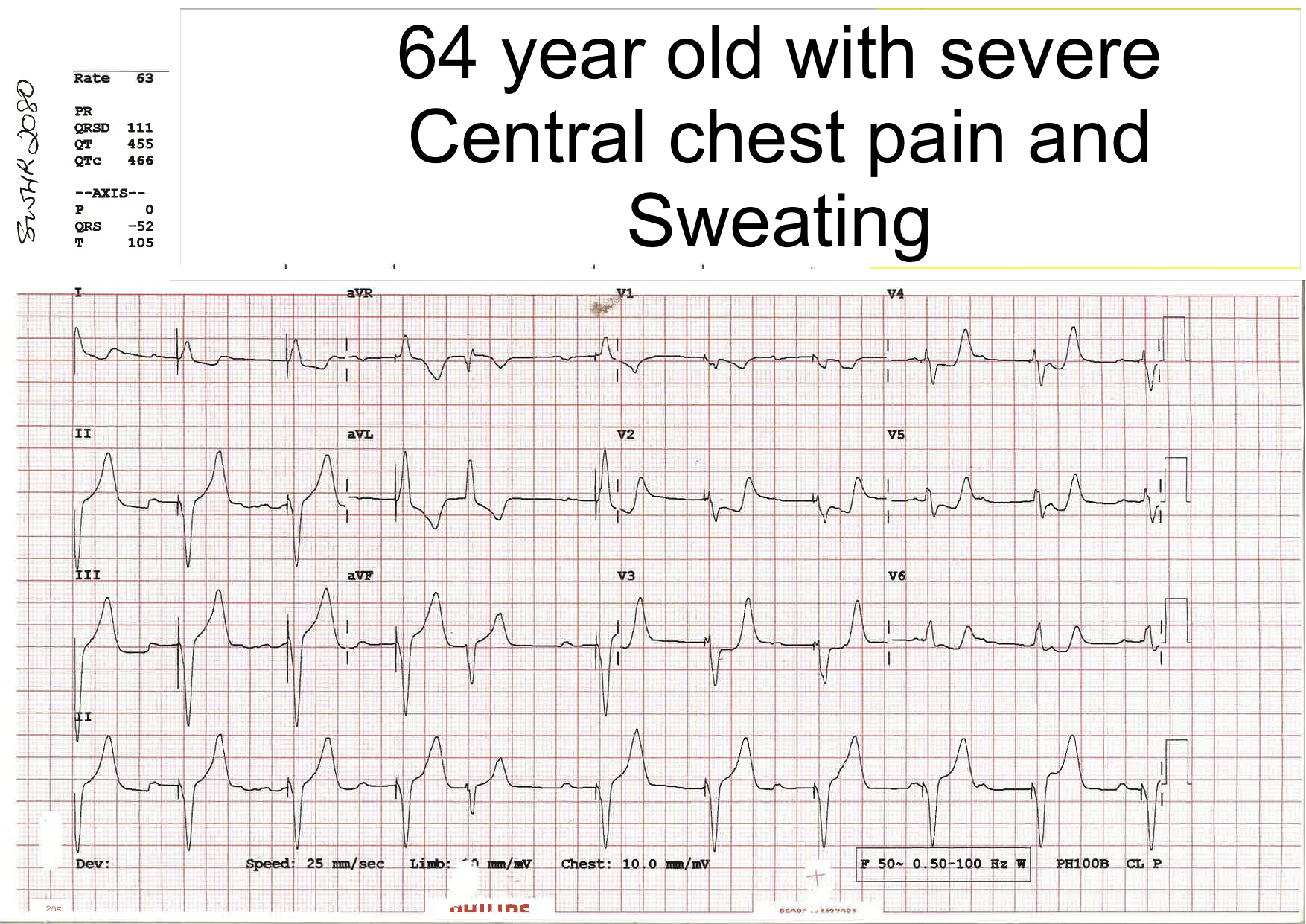
ECG 10 – A 64 year old man with Acute Onset of Chest Pain
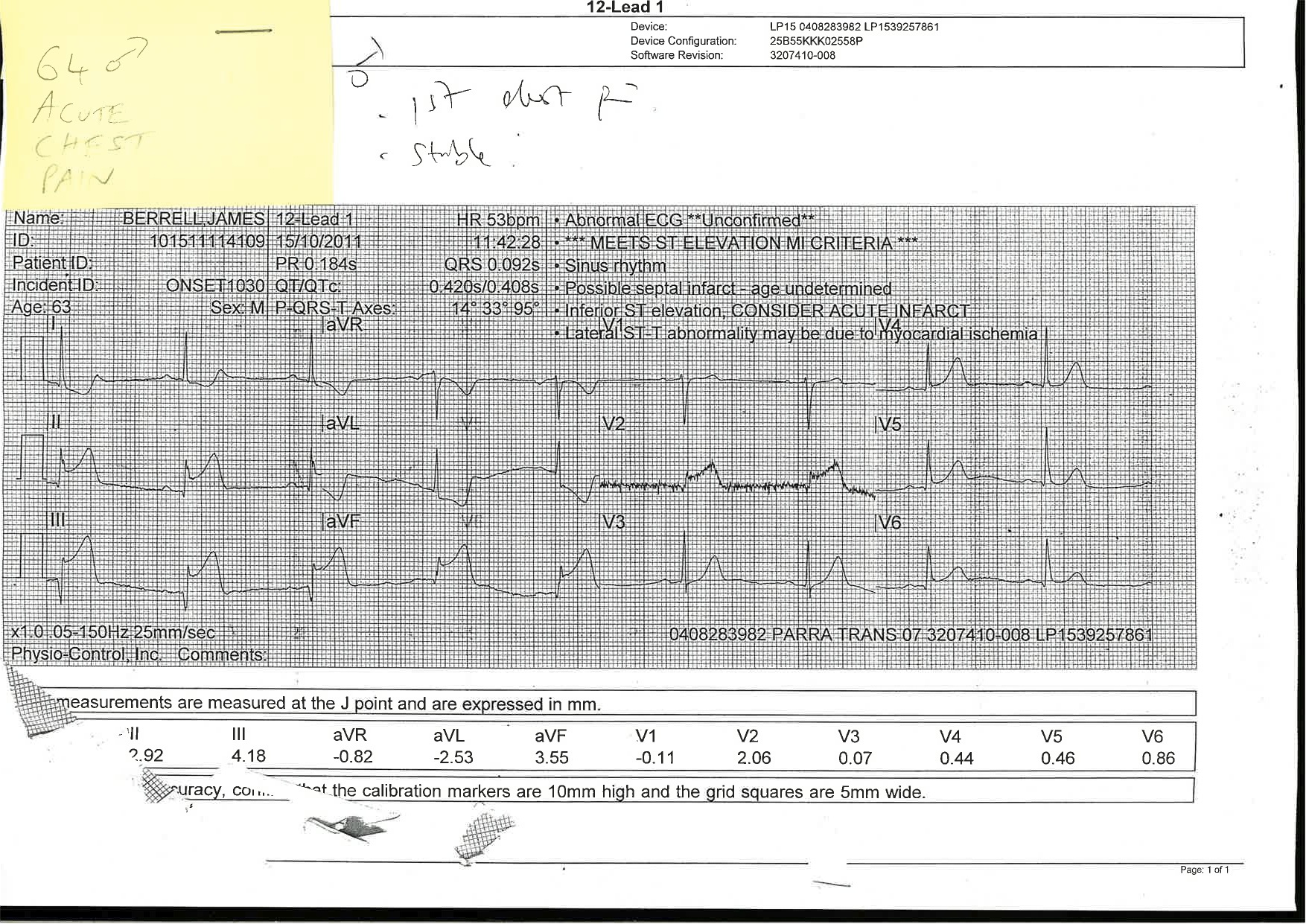
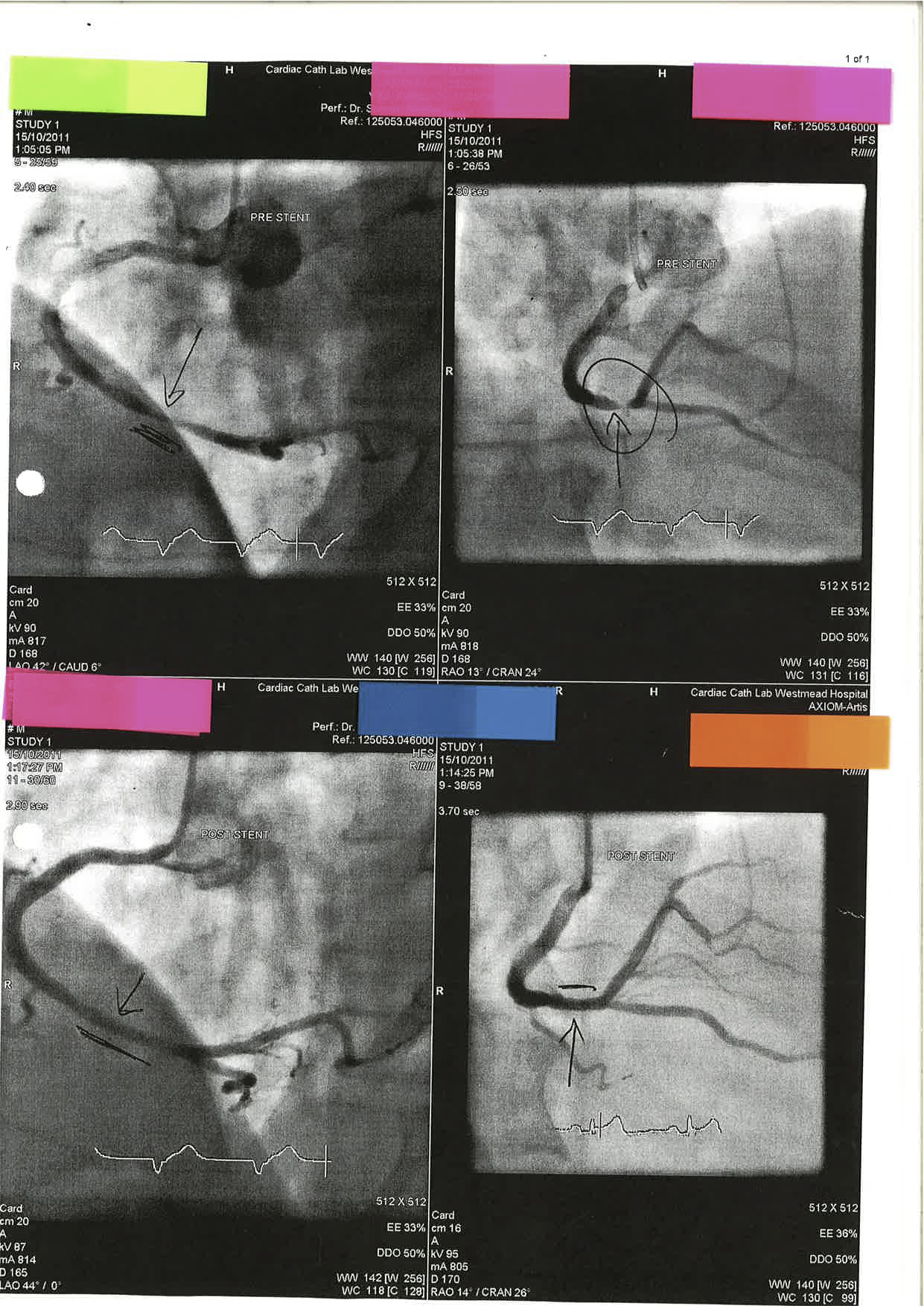
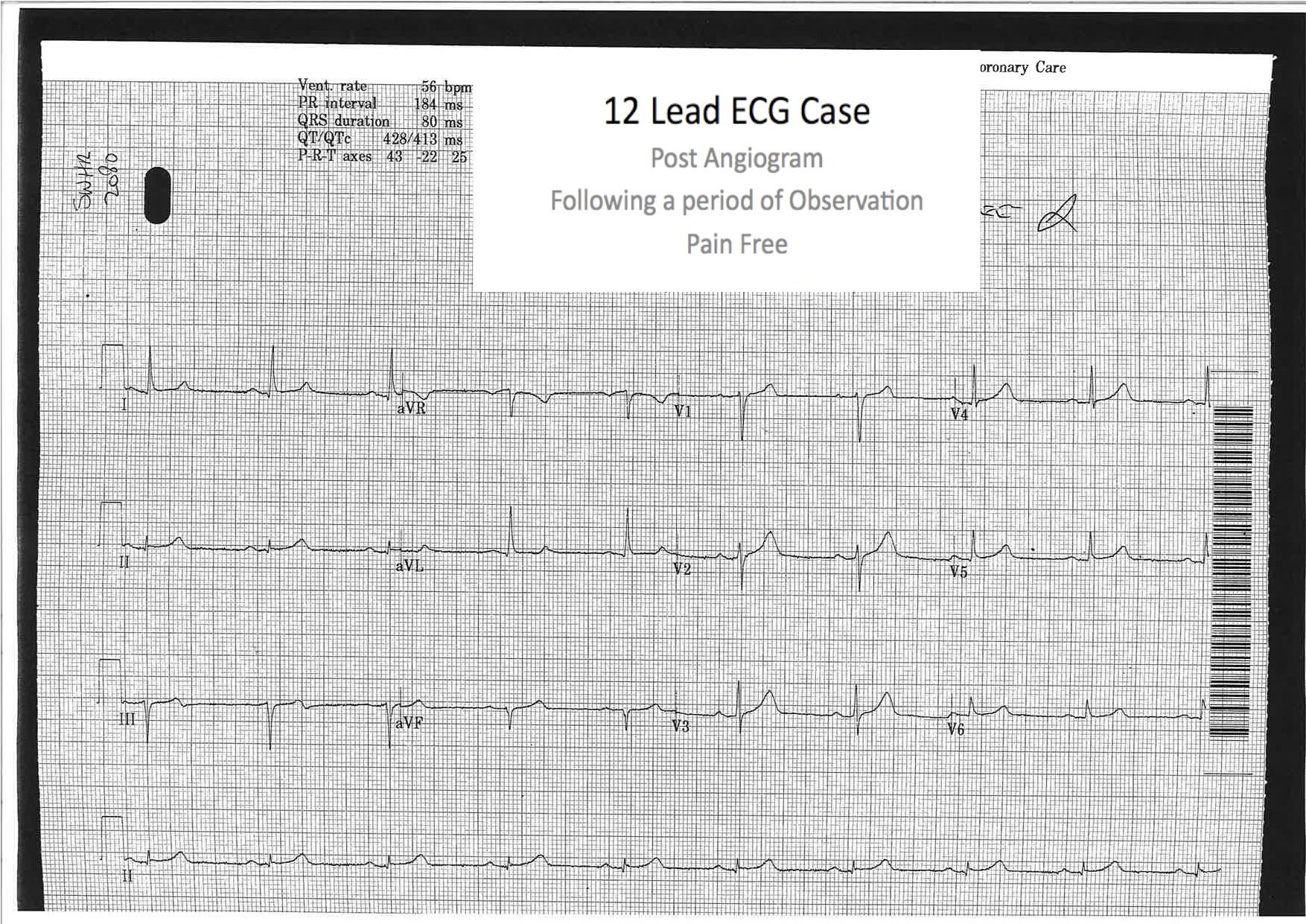
ECG 10 (above) shows inferior ST elevation (III, II and aVF) with reciprocal ST depression in aVL. There are no specifc features of a Right Ventricular Infarction. The patient is sent to the Cardiac Catheter Lab and has the following findings:
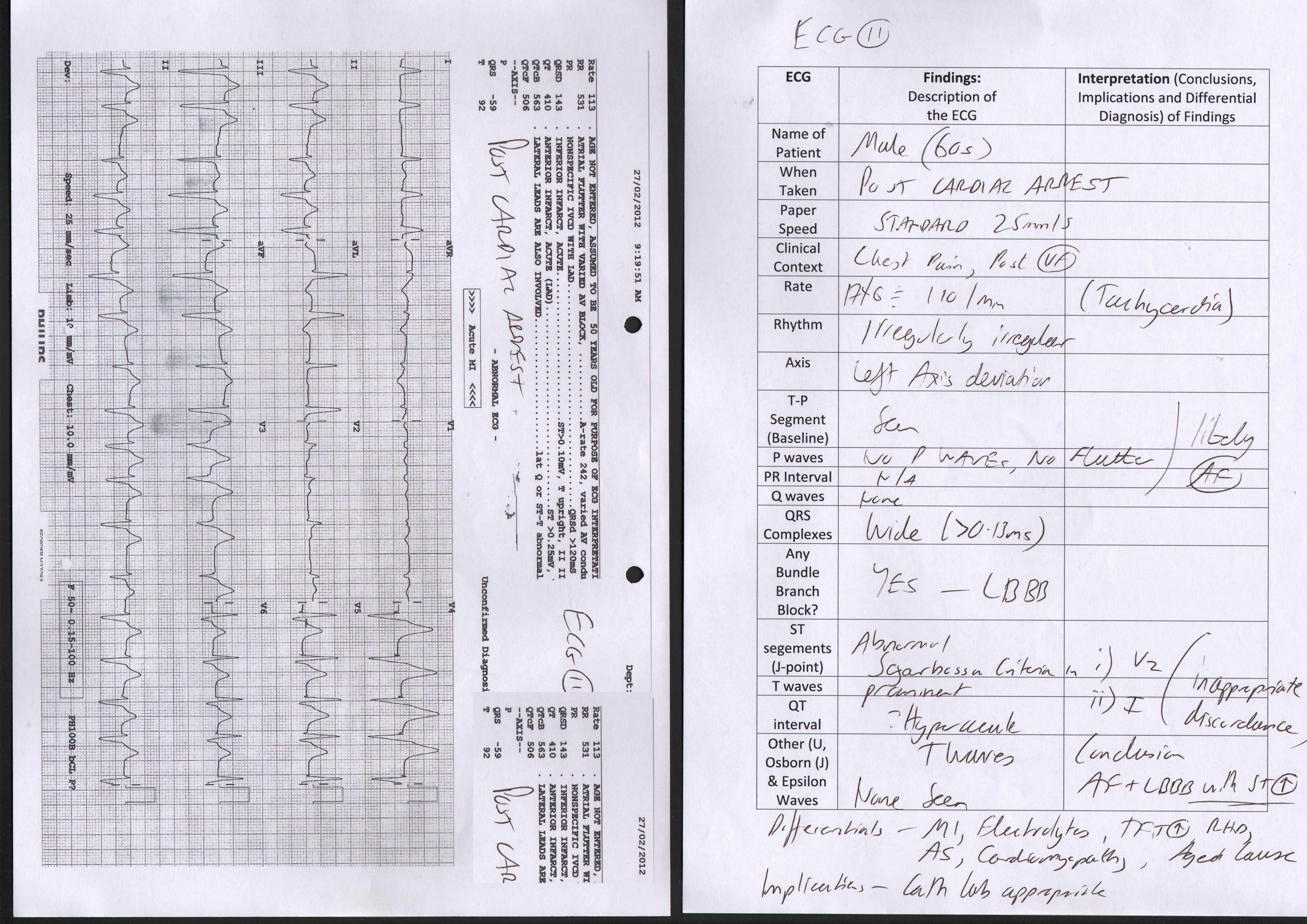
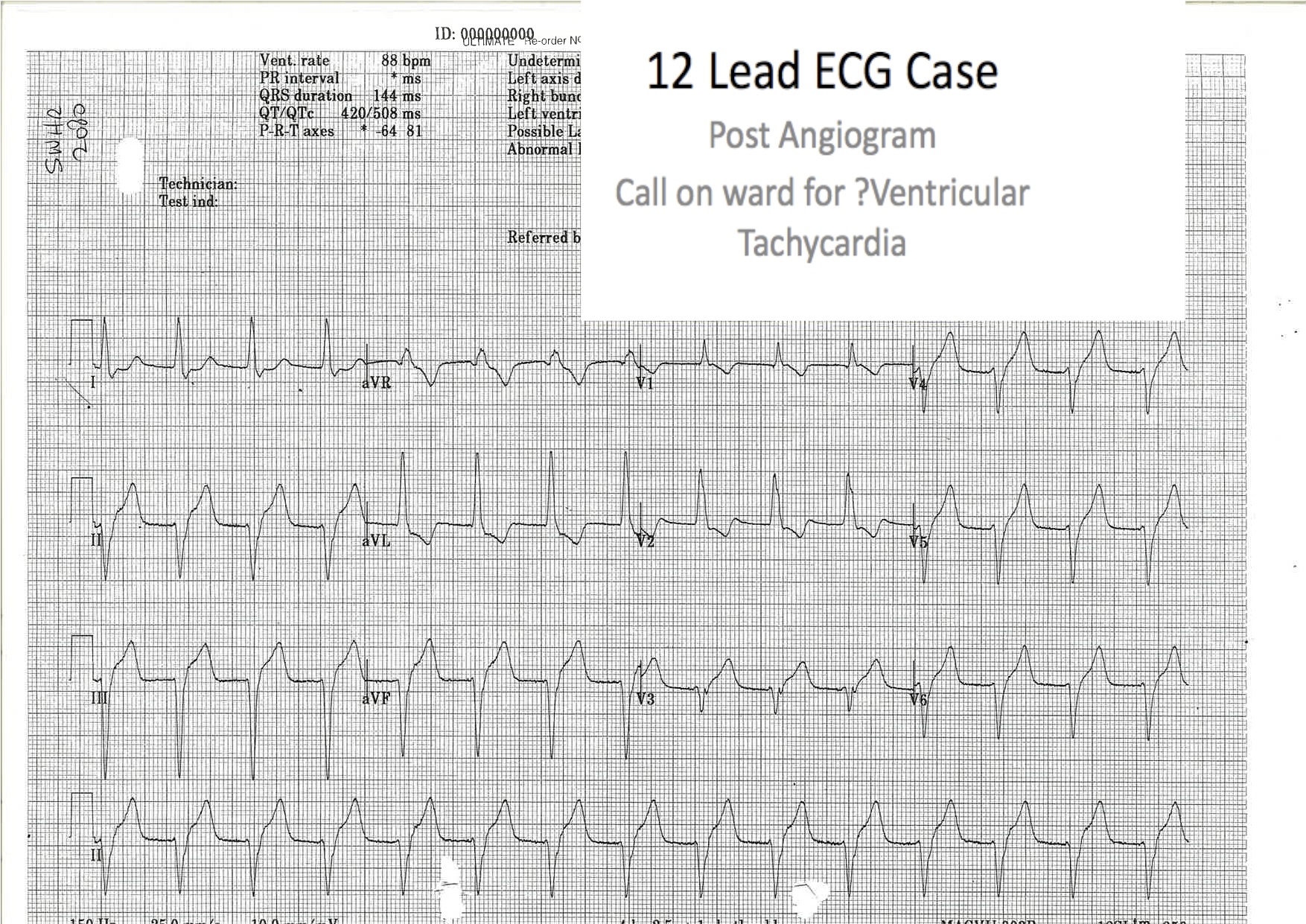
ECG 11 – The patient from ECG 10 has a repeat ECG on the Ward – he is asymptomatic and happy his chest pain has gone away. The nurses are very concerned about the patient having ‘VT’ and have drawn the broad complexes on the ECG to you attention:
Similar cases have been described by Amal Mattu on several occasions:
“Post-MI reperfusion arrhythmias often take the form of a regular, wide-QRS complex dysrhythmia with a rate of 90-120. The rhythm is often mistaken for VT. Treatment with “standard” VT medications is well-known to induce asystole.”
In Summary, in the post MI patient who looks well and has a broad complex arrhythmia be careful not to make a premature diagnosis of ‘VT’ unless the rate is at least 120/minute. A reperfusion arrhythmia if present is likely to be transient and resolve on its own (this was the case with our patient and his follow up ECG is shown in ‘ECG 12’)
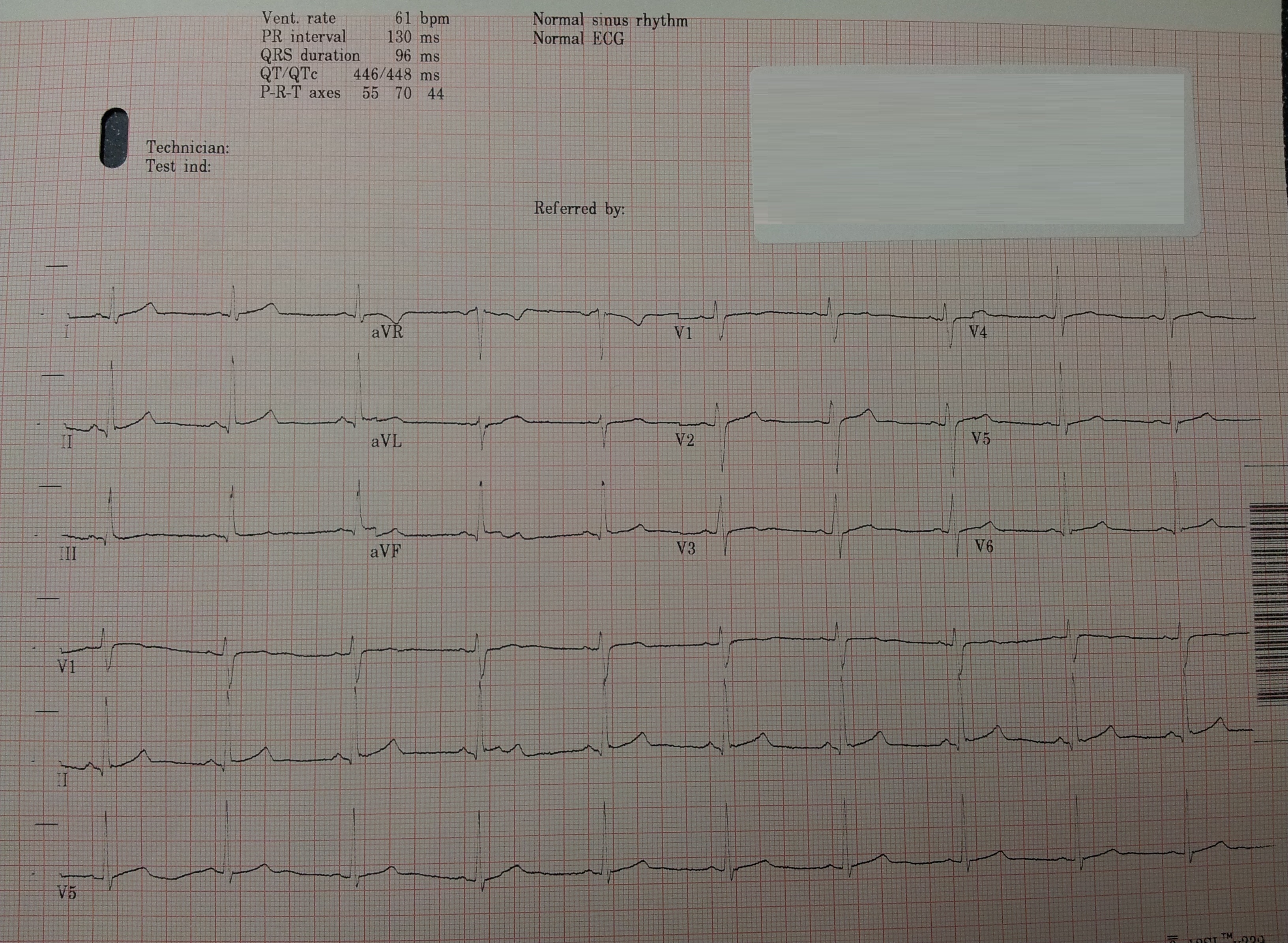
ECG 12 – The patient from ECG 10 and ECG 11 has a repeat ECG taken which shows ‘resolution of the arrhythmia’
ECG 13 – A 13 year old boy has a routine ECG in the Emergency Department
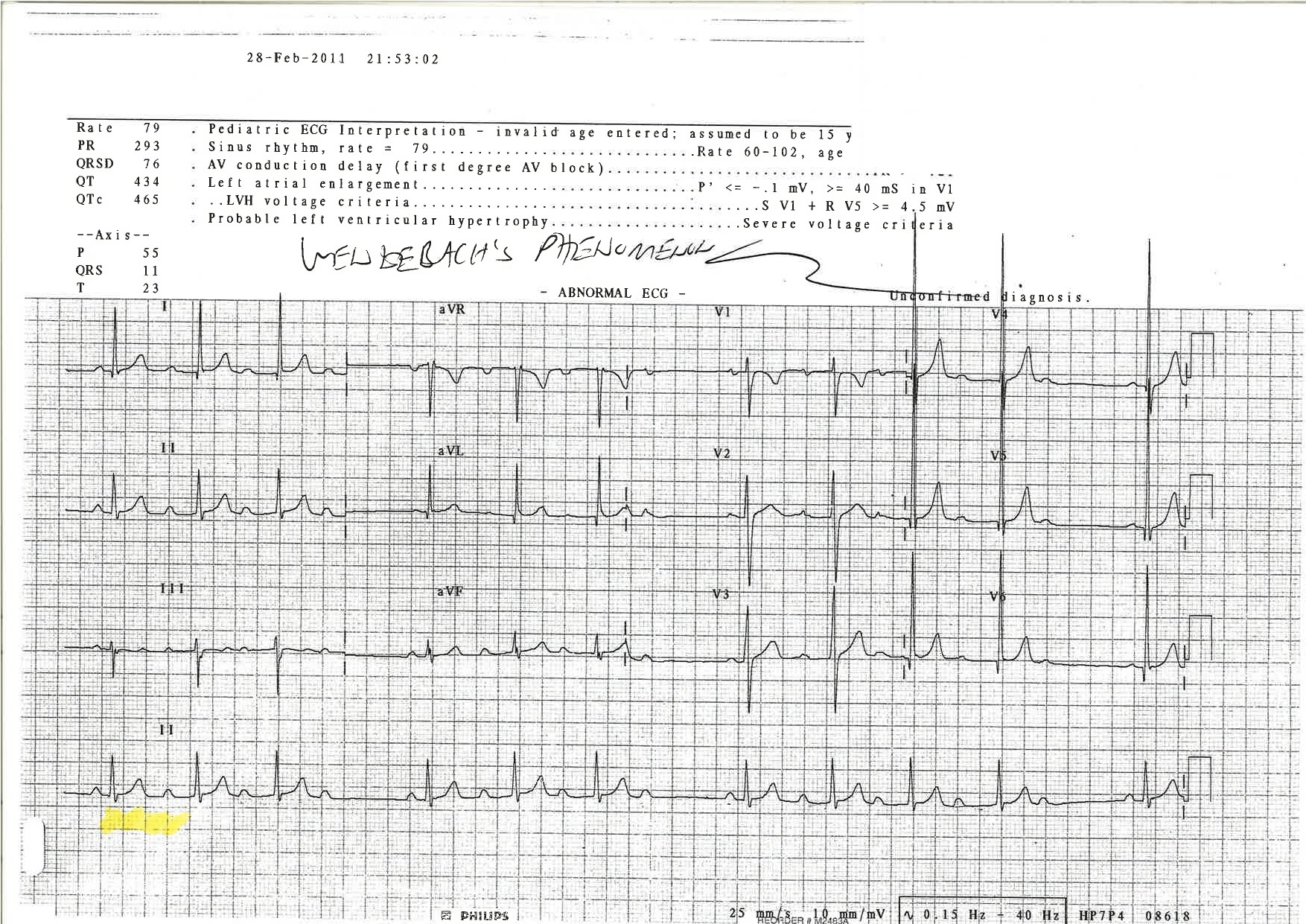
The medical officer reviews the above ECG and diagnosed Type I Mobitz Heart Block (also known Wenckebach Phenomenon). In this case the patient is completely asymptomatic (there is no history of any cardiac symptoms or any family history of heart disease). The case is discussed with the specialist team who asked for a repeat ECG (shown below). After discussion it was decided to reassure the patient and family that Mobitz Type I on an ECG is likely to be a benign finding in children.
However, it should be noted that in patients over the age of 45 that Mobitz I is associated with worsening heart blocks.
ECG 14 – The patient from ECG 13 has a repeat ECG which is shown to the cardiologist
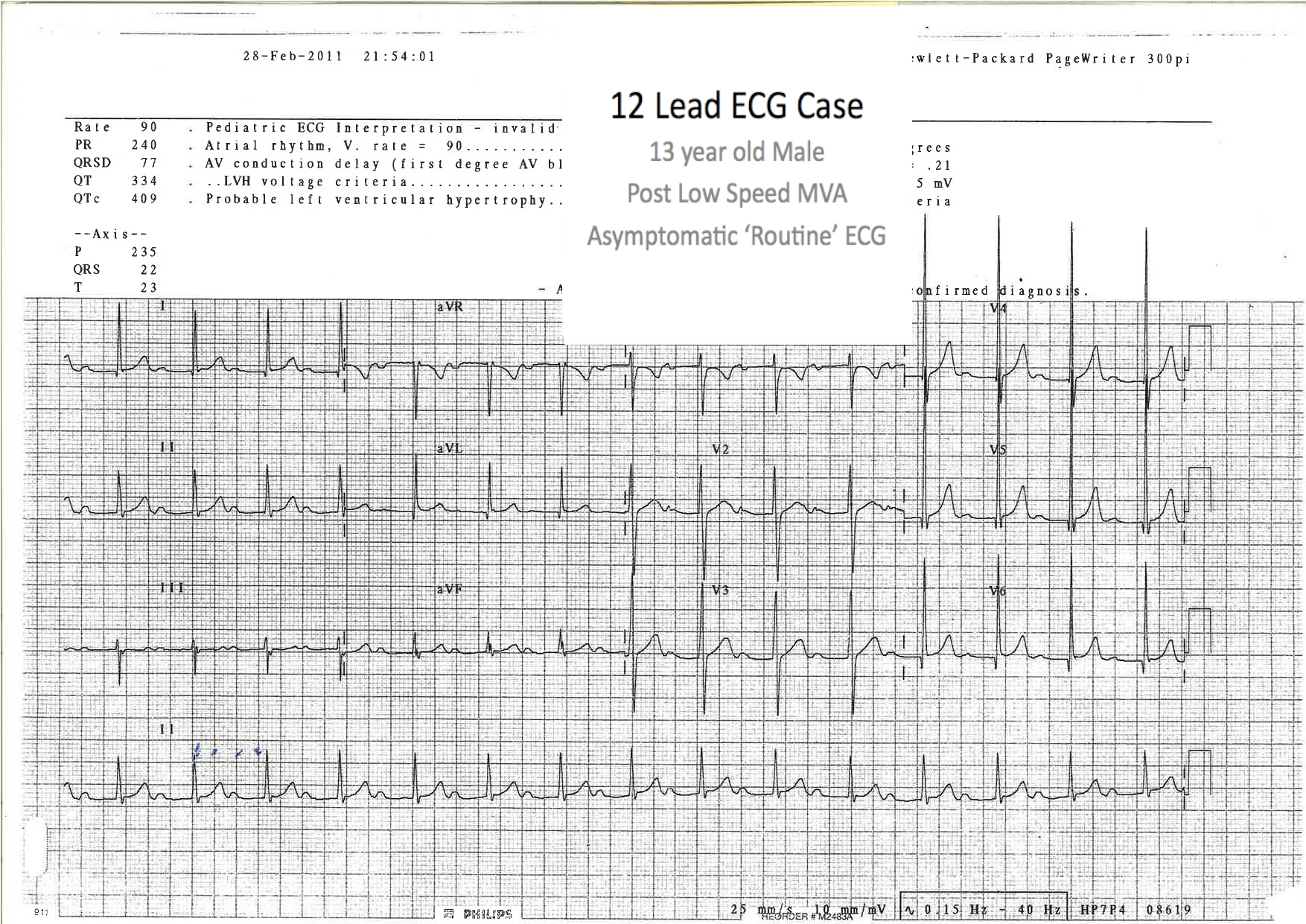
The repeat ECG taken shows a first degree heart block. In teenage boys (this is the ECG of a 13 year old boy) first and second degree heart blocks are more common in athletically trained individuals (found in up to 20% of the population).
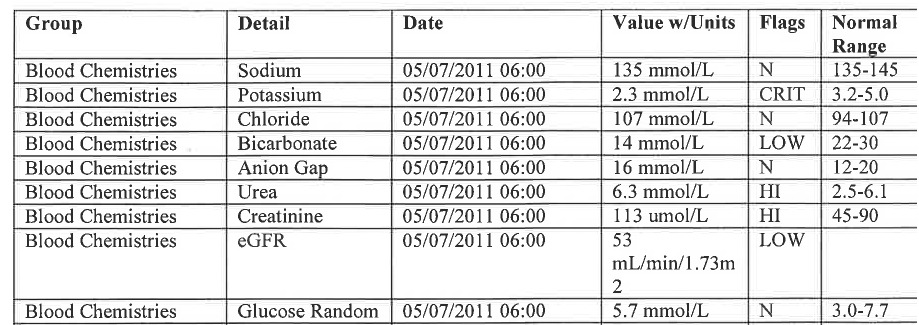
ECG 15 – a 20 year old female presents with lethargy and neck swelling. This is her 12 lead ECG:
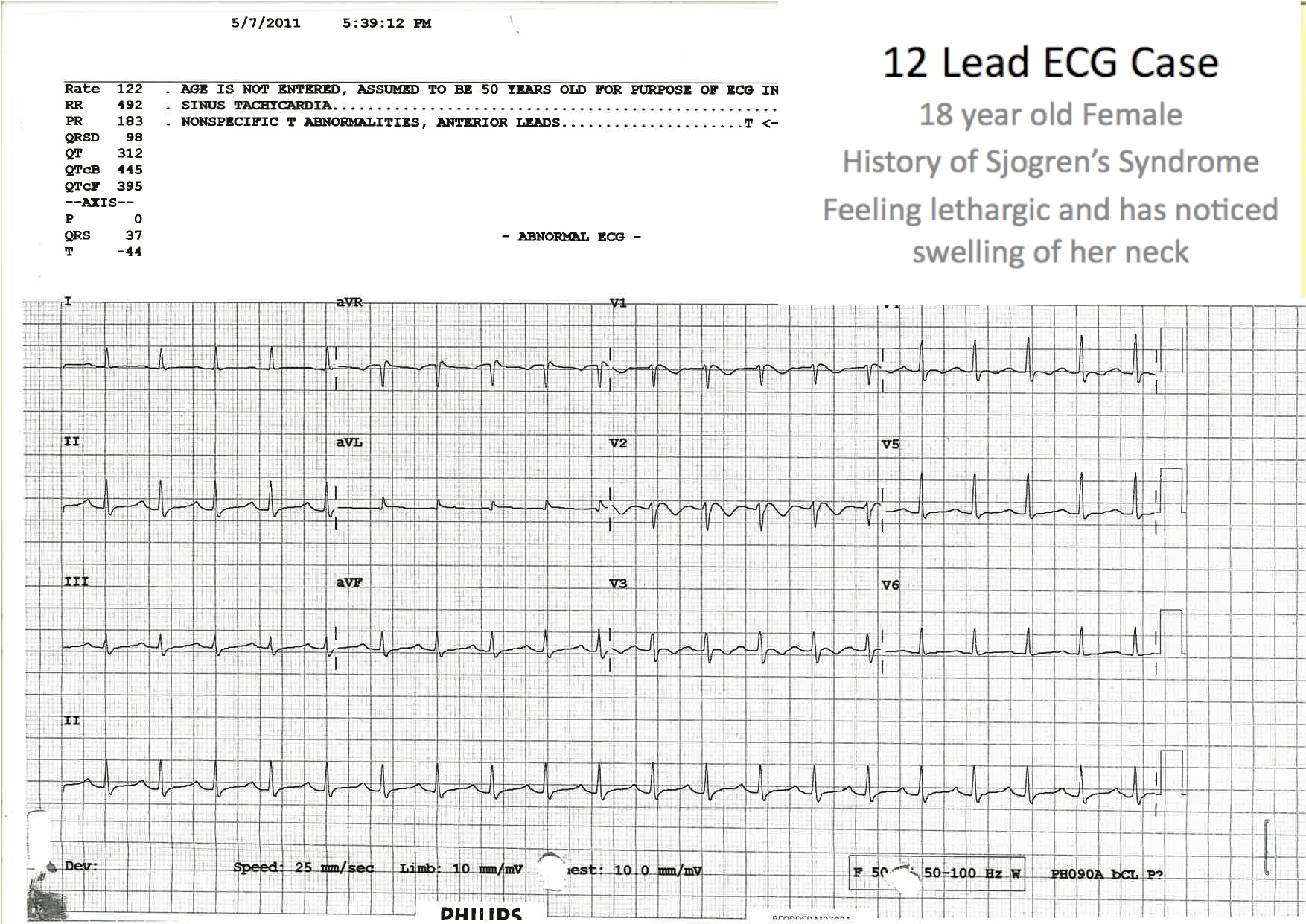
Blood results (shown below) were obtained and she was treated for severe hypokalaemia with potassium and magnesium infusions via a central line placed with USS guidance.
ECG 16 – A patient presents to the ED with Shortness of Breath.
The nursing staff are concerned about his abnormal ECG:
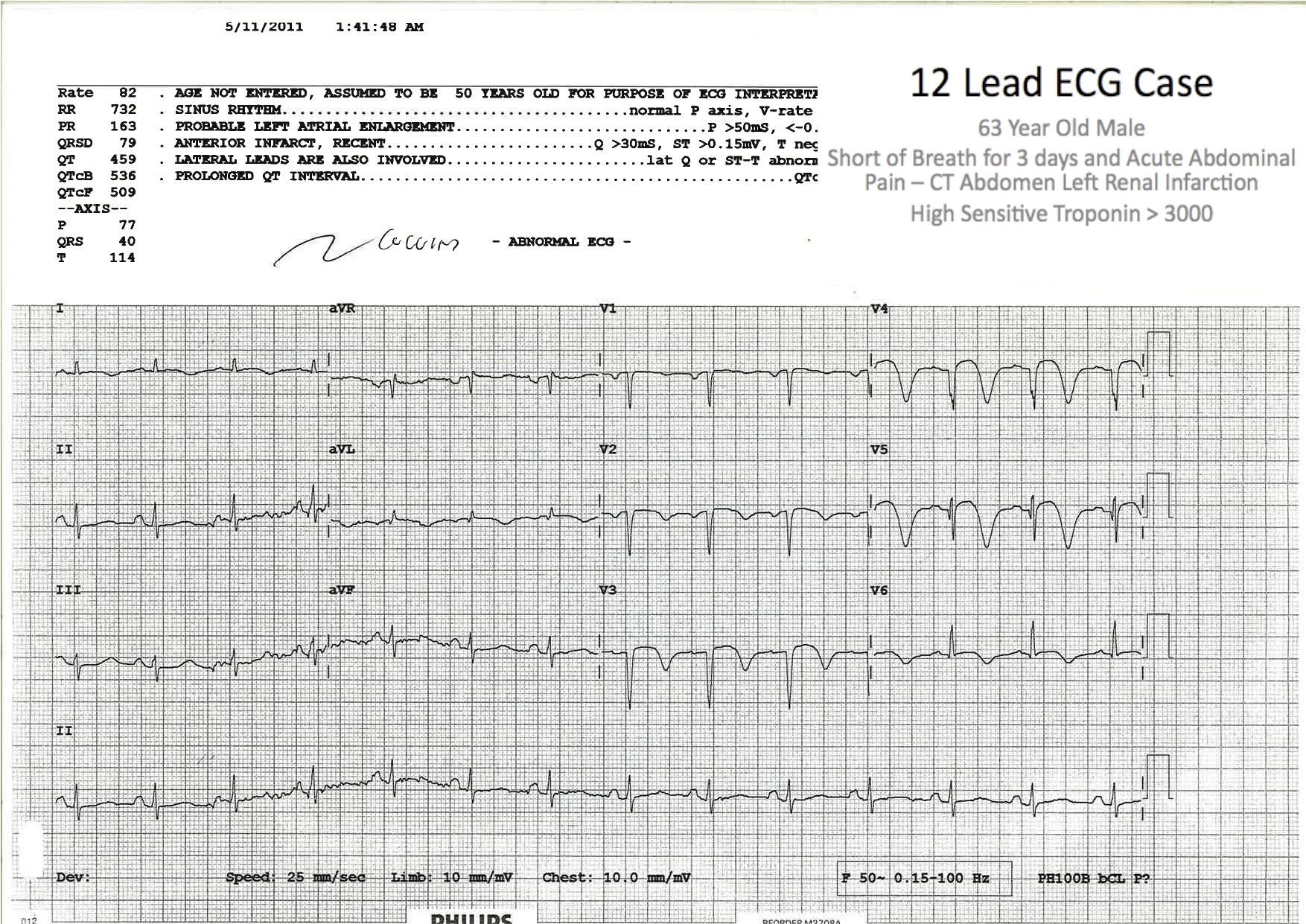
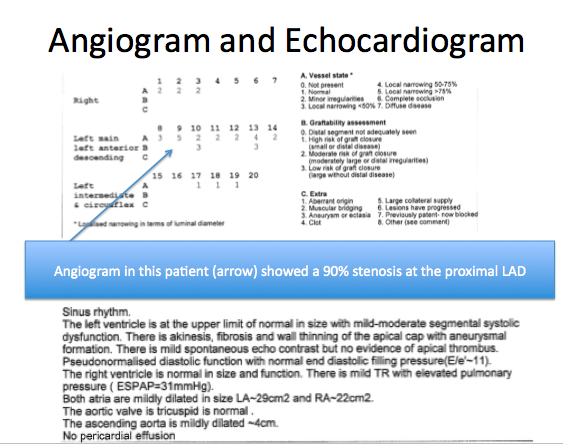
We were concerned following this ECG that the patient may have a cardiac lesion and he was monitored in the ED and referred to the Cardiology team. His angiogram (done within 24 hours) showed a >90% LAD occlusion similar to cases first described by Wellen’s et al with this ECG abnormality.
These findings and mimics of Wellen’s Syndrome are summarised in the following blog:
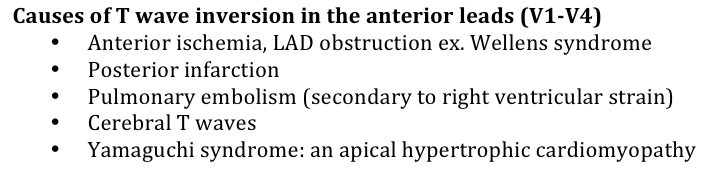
The last two cases have had significant “Anterior T wave inversions“.
What is your differential diagnosis of Anterior T wave Inversion?
ECG 17 – 21 year old male patient with a week of ‘flu like’ symptoms. A 12 lead ECG is taken:

ECG 18 – An 80 year old man presents with Syncope. This is his 12 lead ECG:
ECG 19 – A middle aged patient presents with lightheadedness and a heart rate of 50. This is his 12 lead ECG:
ECG 20 – A 70 year old man presents with fever and hypotension. The patient’s 12 lead ECG is shown:

ECG 21 – A middle aged patient taking ‘heart medications’ presents with palpitations. This is his 12 lead ECG:
A similar ECG was seen in the 2012 FACEM fellowship exam
In high grade blocks (e.g. flutter with 4:1 block) always think of drug toxicity, in particular digoxin toxcity.
ECG 22 – A Middle aged smoker presents with palpitations. They have a heart rate of >160 unresponsive to vagal manoeuvres.
The patient’s 12 lead ECG is shown:
ECG 23 – A 64 year old male with history of Coronary Artery Disease, Cardiac Stents and Pacemaker Insertion presents with chest pain whilst riding a bicycle.
Click Here for a discussion of this case
ECG 25 – A young patient of Asian descent presents with an episode of “loss of conciousness” while lying in a supine position – her ECG is shown

- This is an example of Brugada Syndrome (there are a total of 3 variants) – this was described in the early 1990s by 2 Spanish Cardiologists (they are brothers).
- In Brugada there is RBBB (or Incomplete RBBB). ST elevation (*”Coved“/Saddle type) – this is typically seen in V1-V3 (see video below).
- Presentation with syncope or cardiac arrest is possible in these patients with fatal arrythmia assoicated with a number of genetic channelopathies (up to 20% of sudden cardiac death may be caused by this disease).
- Generally these patients need placement of an Internal Cardiac Defibrillator (ICD).
For the original ‘Brugada Paper’ Click here
More ECG Cases:
ECG Cases for Registrars and Residents
ECGs for TEACHING DOWNLOAD
More cases will be added here in the coming months:
If you have cases your would like to share email andrewrcoggins@gmail.com
