ECG Case Study
Case Study – A 64 year old male with history of Coronary Artery Disease, Cardiac Stents and Pacemaker Insertion presents with chest pain whilst riding a bicycle.
His vitals are normal but he has ongoing Chest Pain and Sweating.
He looks unwell from the end of the bed.

The 12 lead ECG is taken:
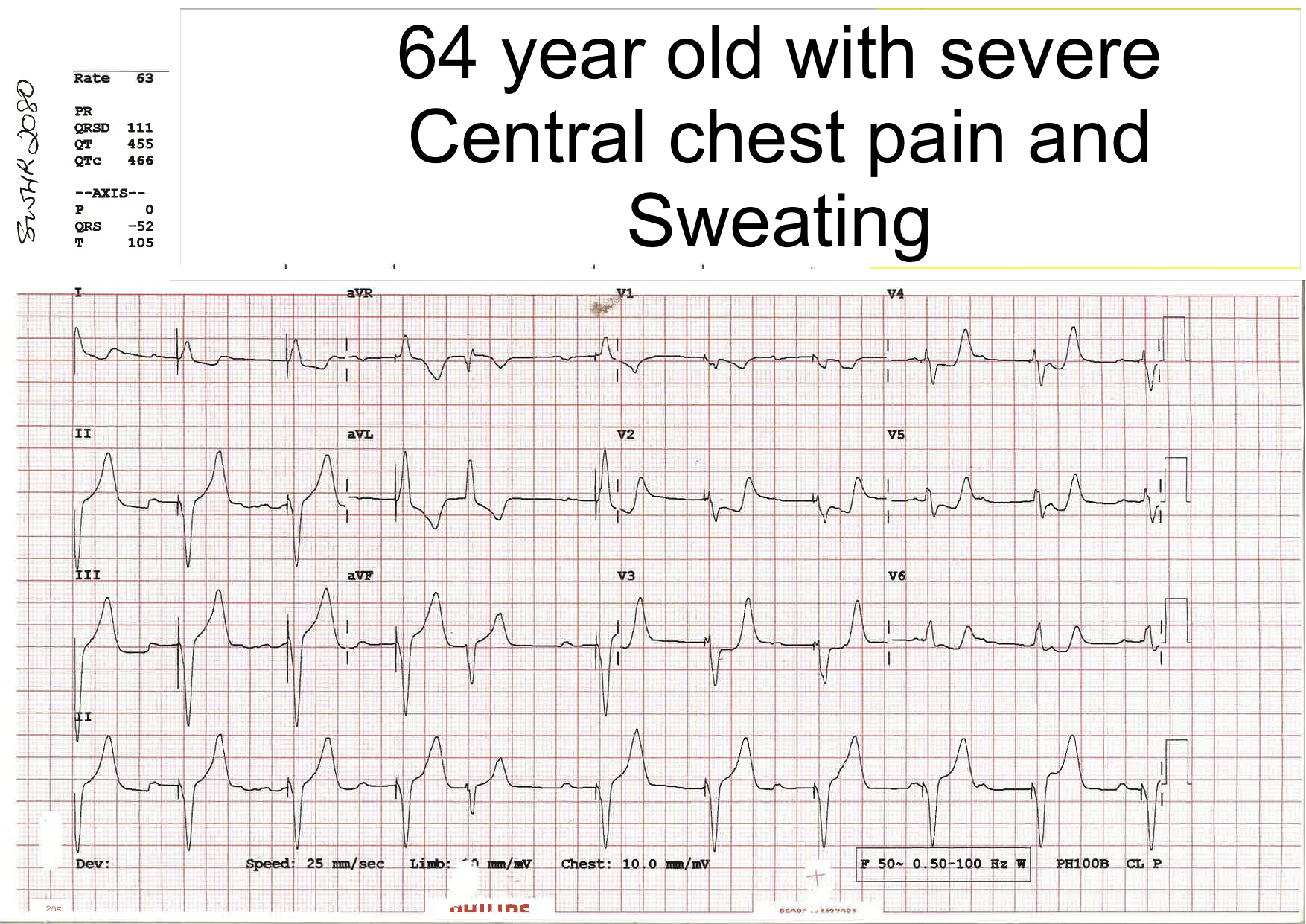
What do you think of the above ECG?
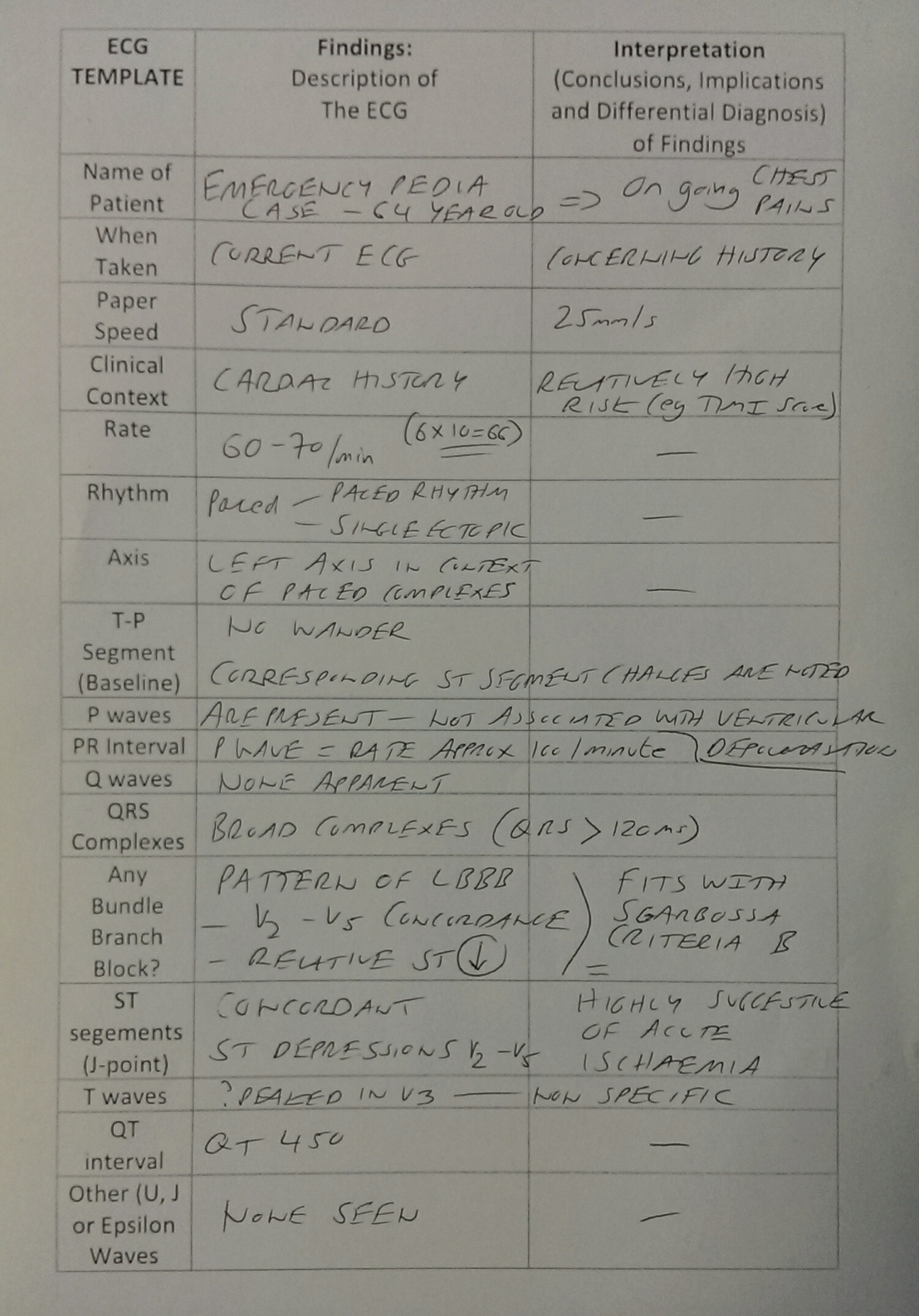
*You can use the Template on our ECG page to describe and interpret the 12 lead ECG*
This ECG was interpreted by the Ward Medical Team as:
“Paced Rhythm – no further comments can be made due to the Paced Complexes“.
However, in this case due to “on-going chest pain” and an interpretation of the ECG by an attending Cardiologist in the context of the clinical history the patient was taken to the Angiography Suite where they were found had significant coronary lesions…
Our Suggested Interpretation
Review of Sgarbossa’s Criteria
The Original Study by Elena Sgarbossa and colleagues was published in the New England Journal of Medicine in 1996. Click on the picture below for a link to the article:

Sgarbossa and Paced Rhythm
While the Original Sgarbossa Paper applied to patients with Left Bundle Branch Block (LBBB), further articles were published relating to the criteria in patients with Paced Rhythm:
The Sgarbossa Criteria in Paced Rhythm
According to the author’s analysis of a small number of patients with Paced Rhythm in the GUSTO I Study (1993), findings of ST segment concordance on the 12 lead ECG (similar to the Sgarbossa’s Criteria for LBBB) were concerning and quite specific for a diagnosis of Acute Myocardial Infarction.
Validation of Sgarbossa Criteria has been questioned in several studies. The changes on the ECG are likely to be specific but not sensetive for Myocardial Ischaemia.
Summary of Sgarbossa Criteria for LBBB
- Originally described as a tool for diagnosing an AMI in the presence of a Left Bundle Branch Block (LBBB)
- Derived from an original study that included over 26,000 patients
- Has often described as “specific but not sensitive”
- Sensitivity around 40%
- Specificity > 90%
- Criticised by cardiologists both in the literature and in clinical practice due to the lack of sensitivity of a single ECG…
- However, even in an ECG with normal conduction, the initial ECG is less than 50% sensitive for the diagnosis of an Acute Myocardial Infarction
- Furthermore, the presence of Sgarbossa’s Criteria has been found to be highly specific for Acute Ischaemia in a number of recent studies
Review of The Original 3 Criteria
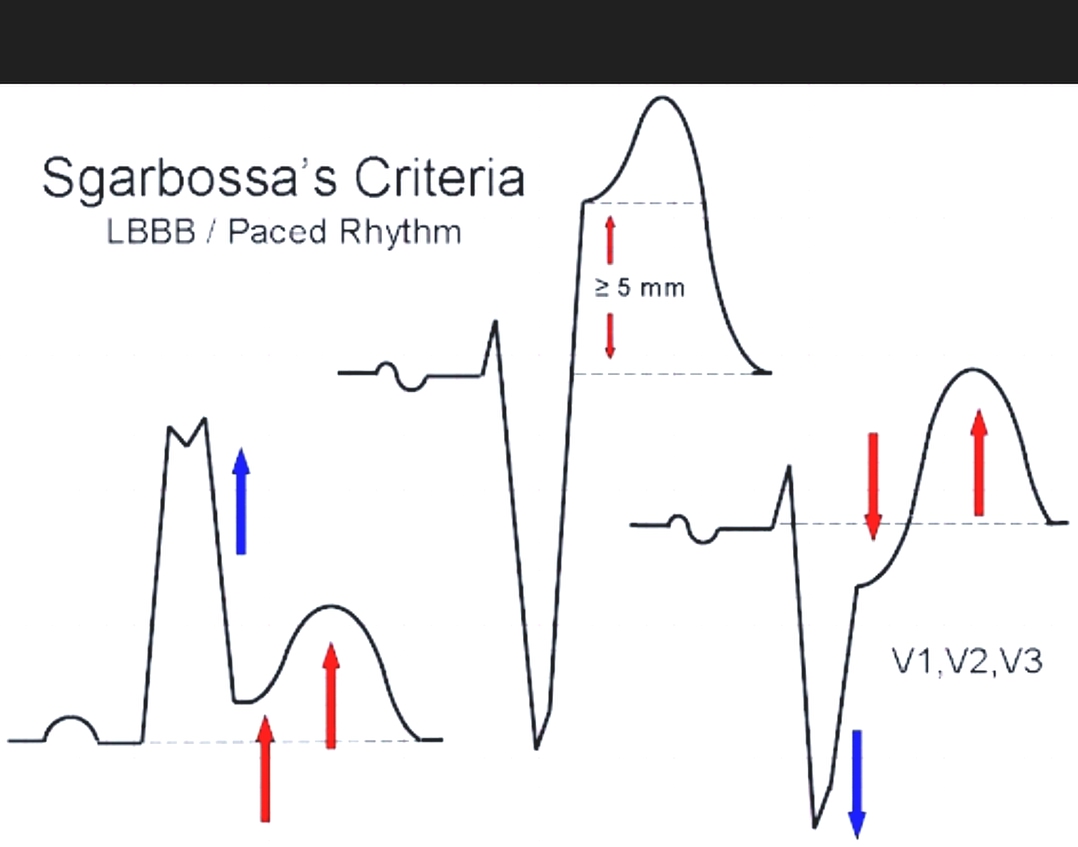
Criteria A
Concordant ST segment elevation of 1 mm or more (V5, V6, I, aVL or II) = 5 points
(About 92% specific)
Criteria B
ST segment depression of > 1mm in leads V1, V2, or V3 = 3 points
(About 96% specific)

Criteria C
Discordant ST segment elevation greater than 5 mm = 2 points
(Less specific)
Criteria C is said to have the lowest specificity of the 3 criteria.
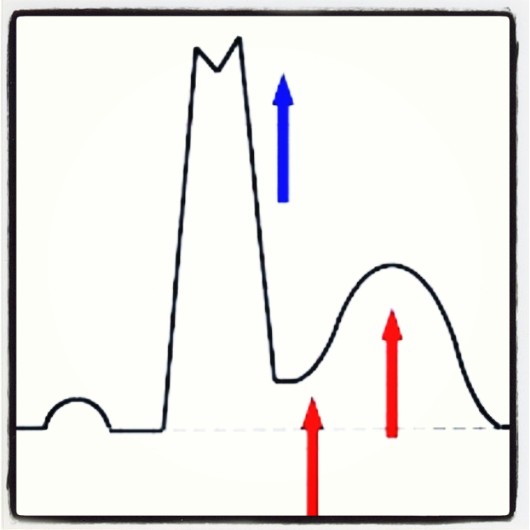
A particular caveat is the depth of the S wave compared to the degree of ST elevation.
Normally, in the presence of a LBBB the deeper the S save the higher the ST elevation… As a result of this proportional amount of ST elevation present in patients with LBBB some authors have suggested that the original Sgarbossa Criteria be amended.
A Modified Criteria could be based on the ratio between the S wave deflection and the corresponding ST elevation. This is shown in the following picture based on Dr Stephen Smith’s description of a Modified Sgarbossa’s Criteria:
Modified Sgarbossa’s ‘Criteria C’

Putting it all Together
A total score of 3 is required to meet the criteria and when present is thought to be specific for Myocardial Infarction. It is worth discussing all patients with a BBB or Pacemaker who have chest pain with a senior colleague in the Emergency Department.
Further Discussion
Validation studies and Review Articles have suggested that a Sgarbossa score > 3 or more has a very high specificity for Myocardial Infarction (>95%) and that there is a higher mortality in these patients than in patients with LBBB associated discordant ST-segment elevation alone (e.g. Criteria C described above).
Dr Michael Kontos and colleagues looked at 401 patients presenting with LBBB and symptoms suggesting an Acute Coronary Syndrome. In this study the authors found:
- 64% of patients presenting were found to have had a new LBBB
- Overall 29% of the patients in the study were ultimately found to be having an Acute Myocardial Infarction (AMI)
- In the final analysis MI was diagnosed in 26% without Sgarbossa Criteria and 86% with positive Sgarbossa Criteria
They concluded that “most patients with possible MI with new or presumably new LBBB do not have MI. Concordant ECG changes were an important predictor of MI and death. Current guidelines regarding early reperfusion therapy for patients with LBBB should be reconsidered“
The Sgarbossa criteria is described in the cardiology literature by Neeland et al who conclude in their paper: “Patients with a suspected ACS in the setting of LBBB represent a much more heterogeneous population than STEMI without BBB and present unique diagnostic and therapeutic challenges to the clinician. Most patients will not have an AMI regardless of LBBB chronicity and likely would not benefit from urgent reperfusion therapy. Current guideline recommendations and performance measures do not account for the evolving epidemiology and complexity of LBBB among patients with possible ACS. We recommend a slightly more judicious approach to diagnosis among hemodynamically and clinically stable patients with LBBB who do not have ECG findings highly specific for STEMI (e.g. the use of the Sgarbossa Criteria)“
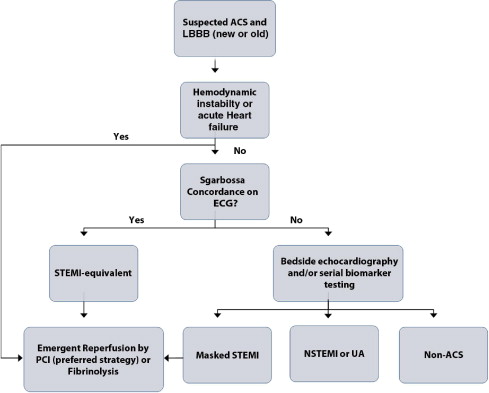
Neeland’s Approach to LBBB in Clinical Practice
Vodcast on The Criteria
ECG Expert Dr Amal Mattu Discusses the Criteria in his Weekly ‘Vodcast’:
Another Case
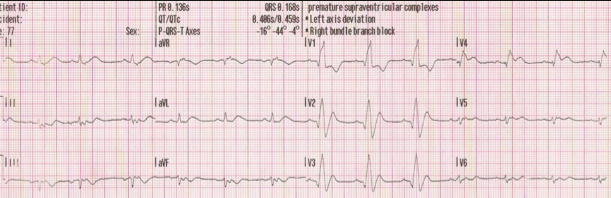
An Example of Concordant ECG changes suggesting rapidly evolving Myocardial Ischaemia is shown below. In this case we extrapolate the principles described above and apply them to an ECG with a Right Bundle Branch Block (RBBB) pattern:
ECG 1
(0 minutes)
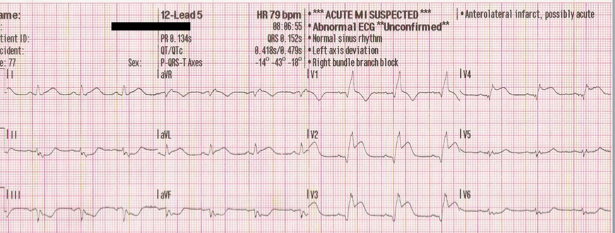
ECG 2
(10 minutes)

ECG 3
(20 minutes)
Take Home Points
Sgarbossa’s Criteria has been shown to be highly specific for diagnosing AMI but must be used in combination with a high level of clinical acumen, follow up ECGs, cardiac biomarkers and use of non-invasive monitoring in the Emergency Department. The criteria can be used in patients with Bundle Branch Block (BBB) and Paced Rhythm.
GIven that LBBB is associated with a high mortality, any patient with chest pain and LBBB should be discussed with a senior Emergency Doctor and/or Cardiologist at an early stage. Where present, the finding of a positive Sgarbossa’s criteria should significantly add to the urgency of activating the Catheter Lab or considering treatment with Thrombolysis.
Another major lesson from the ECGs presented above is that changes on the ECG are dynamic and evolve over time. Therefore, repeat ECGs are important in the Emergency Department for any patient with ongoing chest pain.

Modified Sgarbossa Criteria
– http://academiclifeinem.com/modified-sgarbossa-criteria-ready-primetime/