Case 1
Bradycardia in the Emergency Department
- A 65 year old man presents to the ED with mild chest pain and dizziness following a syncopal episode on the toilet.
- You receive a pre-notification call from the Ambulance: They are concerned about his heart rate of 28…
- His initial ECG shows no specific Ischaemic Changes
What is your differential diagnosis for his Bradycardia?
-
Remember ‘D.I.E.’ – Drugs, Ischaemia and Electrolytes
- Ischaemia is the diagnosis of exclusion – any heart block with syncope chest pain should be closely observed because Myocardial Ischaemia is a dynamic process
- Drug causes include:
- Digoxin
- Non-dihydropyridine Calcium Channel Blockers such as Verapamil
- Beta Blockers
- Clonidine
- Hyperkalaemia is an important cause of bradycardia

In this case the rapid bedside Postassium (venous blood gas) comes back at 8.4mmol/L and the nursing staff are requested to repeat the ECG.
What are the Typical ECG findings in Hyperkalaemia?
Key Point – The ECG may be normal or near normal – a normal ECG is not reassuring. Having said this, ECG changes are common and their presence should prompt a focus on starting specific treatment…
Hyperkalaemia is a time dependent emergency that requires your immediate attention.
Classic ECG Findings
The ECG associated with Severe Hyperkalaemia shows progressive QRS Broadening:


Other ECG Findings
Progressive features suggesting hyperkalaemia include:
- P wave flattening and heart blocks
- An increasingly broad and bizarre looking QRS complex
- Peaked T waves (that often have a pointed appearance)
- Arrhythmia including Asystole (see below) and Ventricular Fibrillation
- The ECG prior to Cardiac Arrest May be normal

CLICK HERE FOR MORE ON 12 LEAD ECGs

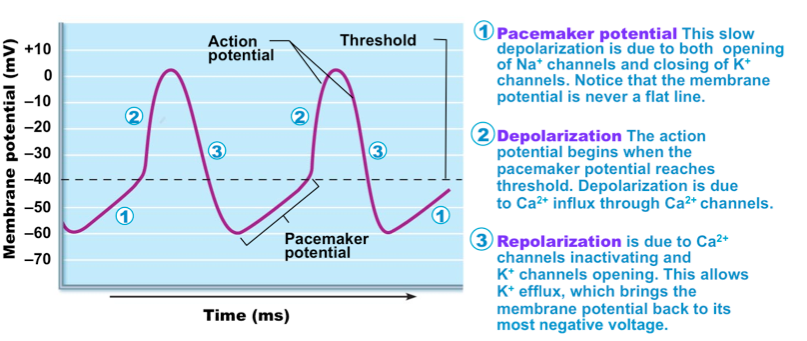
What is the mechanism of bradycardia in hyperkalaemia?
- This relates to the cardiac pacemaker action potential – a reduction in the concentration gradient (outflow) of K+ in repolarisation leads to reduced heart rate.
- The change in serum postassium affects the repolarisation part of the action potential (labelled ‘3’ in the diagram below). Hyperkalaemia leads to a flattening of the angle of this part of the action potential which can lead to a slower heart rate.
How will you manage this Man’s Hyperkalaemia and Bradycardia?
Resuscitation Phase of Care (actions in first 10 minutes)
- Call for assistance and assemble an appropriate team (nursing and medical)
- Move the patient to the Resuscitation Bay (or equivalent)
- Attach the patient to 3 lead ECG telemetry and observe with continuous non-invasive monitoring
- Apply O2
- Position Patient – Sit patient up
- Obtain IV access
- Send repeat bloods (including a bedside point of care VBG)
- Start Intravenous (IV) fluid (e.g. 0.9% saline 500ml/h if not known ‘renal patient’ or a significant risk of fluid overload with small amounts of IV fluid) – this is safe and appropriate in almost all patients
Make a brief initial assessment of the patient:
Blood Gas Point of Care:
A Valuable Tool in the Emergency Department

Specific Treatment
In this case the Undifferentiated Bradycardia may require initial invasive specific management:
(1) Transcutaneous Pacing (usually with Analgesia and Sedation) – may not be effective in Hyperkalaemia
(2) Adrenaline Infusion (Isoprenaline is often now the second line choice due to associated hypotension. Commonly high doses of Isoprenaline are required for an adequate effect)
(3) Atropine Bolus (this is said to be ineffective in most cases. It is more likely to be effective where there are narrow QRS complexes. Atropine can have a paradoxical effect in small doses so if uses make sure you give a decent dose (e.g. 500mcg boluses)
Use a cognitive aid as a checklist of your actions – such as the ALS algorithm for bradycardia
Treat the Cause
Treat the Electrolyte Problem – ‘make the patient safe’ by treating the Hyperkalaemia with IV Calcium
- IV Calcium
- This will NOT lower the total body or serum potassium levels but will reduce the risk of arrhythmia
- May need to be cautious in patients with a high suspicion of digoxin toxicity
- Options for IV Calcium treatment include Calcium Gluconate and Calcium Chloride – 10mls of Calcium Chloride has about 3 times more calcium ions than the equivalent dose of Calcium Gluconate

For more information on calcium – CLICK HERE
Further Management
- IV insulin (i.e. Actrapid)
- 10 units with 50ml of 50% dextrose into a good IV cannula
- Re-check the Blood Sugar at 1o minutes and 30 minutes
- Consider Sodium Bicarbonate (especially with renal failure – but not routinely)
- Consider Salbutamol Nebs (can easily be given – e.g. 10mg nebuliser)
- Consider early consultation for Dialysis (organise early in renal failure patients)
- Document the patient needs a Low K+ Diet
- Fluid Balance Plan Documentation
- Consider Potassium Binders (i.e. Calcium Resonium)
- Proabably not that useful in Acute Management – for more information – CLICK HERE
- Carefully Check the Medication List (stop Slow K plus consider stopping ACE inhibitors, K+ Sparing Diuretics and ARB Blockers) – see the Medical Students Page for a discussion of how to avoid prescribing errors…
- Checklist of Supportive Care Measures – e.g. FASTHUG
- See Previous Post on ‘FASTHUG’ – CLICK HERE
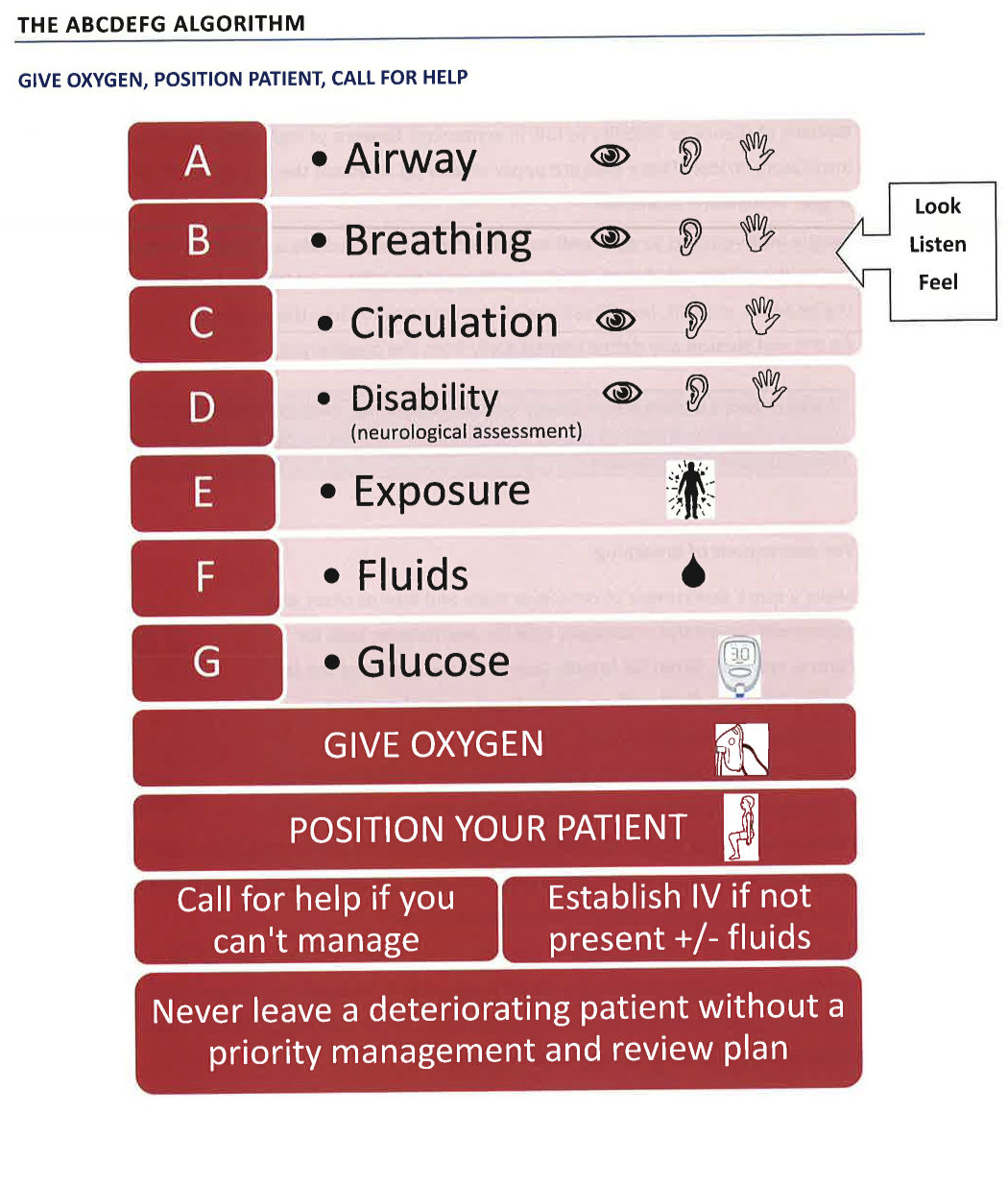
- Reassessment of the patient using a ‘ABCDEFG’ approach described above
- Explanation and Advice to Patient and Family
Disposition
- Need to liase with Dialsysis Unit – may require urgent dialysis
- Consultation with Renal and/or Endocrine Team
- Document the aims for fluid balance
- Admission to hospital
- A monitored bed (continuous ECG) with regular re-checks (i.e. 4 hourly) of both Sodium and Potassium levels
