
EmergencyPedia is part of a family of critical care blogs based on the values of Free Open Access Medical Education (FOAMed). We mourn the passing of SMACC and the FOAMed world’s hero Dr John Hinds who sadly died in early July 2015. This Blog is dedicated to supporting his memory and legacy.
Our team hopes that our website will be useful to medical students, nurses, paramedics, allied health and doctors. In 2015 we will continue to add more content on topics relevant to Emergency Medicine (EM) with our goal being to provide a high quality medical education resource.
We believe in online medical education and that the sharing of our crisis management experiences is the best way to improve our future practice. Reflecting on cases is the best way a young resuscitation practitioner can improve their future care.

The EmergencyPedia team are always interested in your feedback and we are active on various social media platforms:
![]()
![]()
Why become a ‘Resuscitationist‘?
Why become an Emergency Physician?
Why Learn Resuscitation?

Our ‘FOAM’ Favourites
(Click on the Icons to check out these great sites):
![]()




Nice Job – Great Site
Looking forward to SMACC in Chicago 2015!!
– REBEL EM have summed up the fantastic SMACC experience – http://rebelem.com/social-media-critical-care-smacc/
Hey Andy,
I am a paramedic student and I have some questions about the pathophysiology of ACS. Also what is the difference between ACS and AMI?
Lorrie 🙂
P.s. Chicago is UNREAL!
Hi Lorraine – thanks for the comments!
I think that your question about Acute Coronary Syndrome (ACS) is a common one.
To answer with brevity – any patient with significant Cardiac Chest Pain (chest pain from narrowing of the coronary arteries) has ACS.
ACS is sub-divided into 3 further ‘syndromes’ that have overlap in terms of their pathophysiology and presenting symptoms.
These 3 ACS sub groups are treated historically differently. The first two of the three sub-groups are types of Myocardial Infarction (Acute MI) known as Non ST Elevation MI or ST Elevation MI. ST Elevation is detected and diagnosed on the Electrocardiogram (ECG).
The 3rd sub type of ACS is known as Unstable Angina. Unstable Angina has the same underlying pathology as NSTEMI but without detectable death of cardiac cells (we determine this in the ED by measuring various cardiac enzymes such as Troponin).
So to answer your question directly – MI is cardiac cell death due to coronary occlusion and ACS is coronary occlusion causing symptoms such as chest pain with or without permanent damage to the heart muscle cells.
What is the reason why a distinction has been made between NSTEMI and STEMI? Well, this has been seen as important because active re-perfusion therapy has improved survival in patients with ST elevation on the 12 lead ECG. ST elevation is suggestive of coronary artery occlusion due to ‘plaque rupture’. This is (in theory) is readily amenable to treatment with re=perfusion therapies. Re-perfusion can be achieved either Thrombolysis drugs or an Invasive Cardiac Intervention known as Angioplasty. Despite the separation of NSTEMI and STEMI many patients with NSTEMI have complete blockages that would normally be associated with a STEMI when the cardiology doctors do an angioplasty/angiogram so the two conditions are not truly separate entities – they have the same underlying cause.
Wow! Great response. I understand what you mean. In regards to q wave elevation, with NSTEMI, there is no q wave elevation, so what are the typical ECG signs of a NSTEMI ?
Lorrie
Hi Lorrie,
I think you are getting confused between Q waves and ST segments.
Q waves can develop on an ECG several hours after an AMI and may become a permanent fixture of that person’s ECG. Q waves do not show elevation.
STEMI = ST Elevation Myocardial Infarction
NSTEMI = Non-ST Elevation Myocardial Infarction
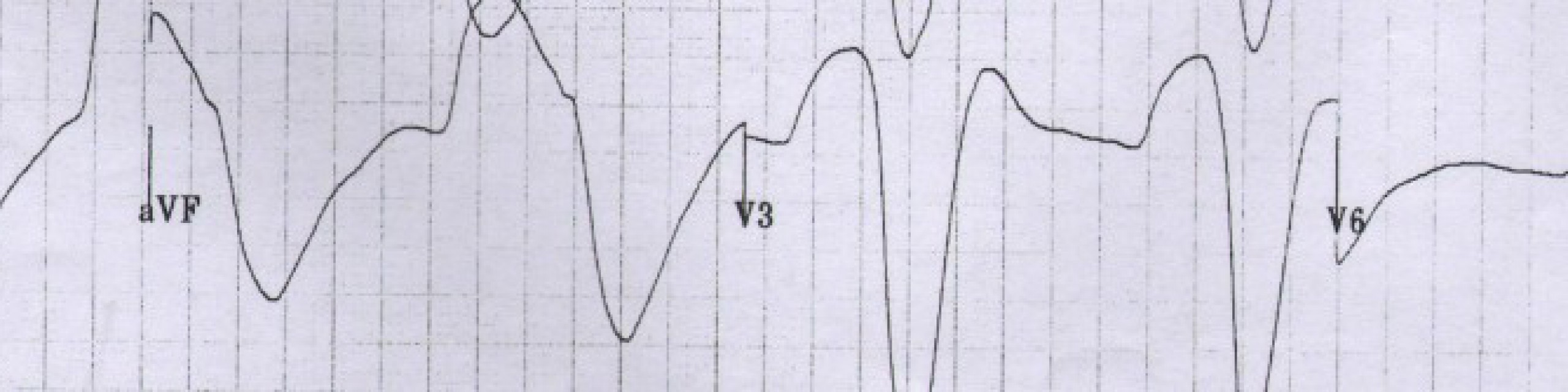
So NSTEMIs will have no ST elevation on their ECG. They may have ST depression, T wave inversion or no changes. They will however have a positive troponin result indicating due to ischaemia to the cardiac cells.
Cheers,
Stuart
Hi Dr Coggins,
I’m Raz, the medical student who attended the Emergency Management Airway Workshop yesterday and asked about oxygenation during a cricothyrotomy. I’ve been taught by an anaesthetist to oxygenate for 4 seconds initially and release, and re-oxygenating if the saturation drops for 2 secs consecutively.
This is a different approach when comparing to oxygenating for 1 sec and releasing for 4 secs, and was wondering if this is also accepted widely and if there will be any significant impact/difference?
Raz
p.s – This blog is superb will definitely recommend it and spread the word
Hi Raz.
Thanks for the comments and the question during the airway session
– the airway workshop post reading will be up shortly
Regarding your questions:
– The Jet Insufflation and Needle Cricothyroidotomy techniques are well described – http://www.ncbi.nlm.nih.gov/pubmed/10593796
– There is a nice review of this on EMCRIT – http://emcrit.org/blogpost/more-needle-cricothyrotomy
“Specifically, 30 to 63 kg ruminants with an obstructed upper airway were resuscitated for 30 minutes from a hypoxic, hypercarbic, and acidotic state using 12- and 14-gauge catheters connected to a 50 psi oxygen source via a two-way valve with an I:E of 1:4 and 1:9 seconds, respectively. Shorter expiratory time or increased inspiratory time with these intravenous catheters resulted in significant hemodynamic compromise, barotrauma, inadequate carbon dioxide elimination, acidemia, and frequent death.” Link – http://www.ncbi.nlm.nih.gov/pubmed/2331256
More Information:
– According to this Paediatric Review Power Point you need to allow the lungs to deflate for 4 seconds https://www.apls.org.au/sites/default/files/uploadedfiles/Failed%20Intubation%20-%20Philip%20Ragg.ppt
– However, I can see why an anaesthetist might say you need to use Jet Insufflation for as long as it takes to move the oxygen saturations in the right direction. We must take care to not leave “On” the oxygen indefinitely as there have been reported complications from leaving oxygen on using a closed circuit – https://www.scotcourts.gov.uk/opinions/2010FAI15.html
Summary – there is likely to be a risk of significant barotrauma from any of these high pressure airway rescue techniques if you leave the 02 on for extended period. The evidence is limited to low levels of experience from experts and from animal studies
Hope this helps
Kind Regards
Andrew
Here’s the workshop summary – https://emergencypedia.com/2014/10/12/airway-workshop-medical-students
Thanks for coming