
Disaster Medicine
The Emergency Medicine Interest Group (EMIG) are organising an upcoming education event on “Disaster Medicine” presented by Dr Kavita Varshney
This EMIG Event will be on the 24th of July at 4.30pm – Westmead Hospital Education Block (Level 2)

Disaster Medicine Review
Here we review the basics of Disaster Preparedness and Planning:
(1) What are the General Considerations for Disaster Situations in the Emergency Department (ED)?
- Firstly, this is a Challenging Situation:
- Dealing with Multiple Casualties which is challenging from a medical point of view (both major and minor presentations)
- There are Crew Resource Management (CRM) issues for the treating ED team including communication, working under stress and leadership
- The team may have little or no experience at dealing with a disaster scenario
- Triage – we should make the switch to a pre-designed form of ‘Disaster Triage’
- Disaster Declaration – An Early ‘Call for Help’ – declaring a disaster and mobilising additional resources
- Types of Disaster
- Disasters can be ‘SIMPLE’ (isolated incident where local infrastructure is not damaged) or ‘COMPOUND’ (infrastructure is limited or damaged by the event)
- Disaster Management Principles
- Planning is a key consideration:
- An ‘All Agencies Approach’
- Integrated Emergency Services
- This approach recognises that no single agency can prepare for and deal with the disruption to community life and infrastructure that can result from a disaster.
- All ‘Hazards’ Approach
- This approach assumes that the functions and activities applicable a single hazard also apply to a range of other hazards. Therefore, a disaster response will involve some tasks applicable to all hazards.
- ‘Comprehensive Management‘ (Planning, Response, Recovery)
- Organisations e.g. SPHERE – www.sphereproject.org have relevant resources in regards to the various phases of a diaster response
- ‘Community Preparedness‘, Training and Education
- An ‘All Agencies Approach’
- Planning is a key consideration:

You are the first on scene at a major train crash and are about the call the Emergency Services:
What are the initial key priorities?
- Safety of yourself before all else
- A brief assessment of scene
What information should you provide over the phone?
The ‘METHANE’ Handover is an appropriate approach in this situation:
- The M.E.T.H.A.N.E. handover from the scene:
- Major Incident, Exact Location (GPS or Cross Streets), Type of incident, Hazards, Access, Number of Casualties, Emergency services required at the scene
- Why is the METHANE Handover useful?
- Activation of Disaster Response and of an Internal Disaster Plan (of the ED and Hospital)
- This will allow planning of resources required in response
- Where possible give your number to the operator and use GPS or cross streets to confirm location
The Emergency Department is asked to send a team to the scene of a disaster.
What are the considerations?
- Personnel (may include nursing, medical and allied health professionals) – a medical commander should lead the team and they are in charge of liaison with other emergency services at the scene)
- Equipment (pre-prepared packs, all weather clothing, identifying tabards and appropriate footwear)

- Transport (to and from the scene of the disaster)
- Communication (including lines of communication, phone numbers, NOK)
- Command Structure**
- Actions at Scene – Sort/Sieve (Triage), Emergency Treatment, Use of Resources
- Relief (both of the ED team and gaps in the roster for the hospital)
- Debriefing (hot and cold debrief)
- Post Incident Care of Staff
** In terms of command and control structure there is a well established chain of command that needs to be followed:
- The Police are in charge of scene of the disaster in close liaison with Fire Services.
- Medical Personnel need to report to the Medical Commander
Your team has arrived at the scene – what are your actions now?
Medical Team Actions
- Medical Team establishes a ‘Casualty Clearing Station’
- Safety of Self, Other Rescuers, Scene and Survivors are all important
- Prioritise and Plan transport Needs – apply temporising treatments only
- Communication – 2-way, runners, phone, direct, closed loop communication and radio
How is the Casualty Clearing Station set up?
Establish Casualty Clearing Station
- Controlled Access
- Up-wind, Up-hill of Site
- Flat Ground
- Cover (ask for Assistance), Power, Equipment
- Separate areas for Walking and ‘non’ walking
- Communication with Command Centre
- Signage, Ambulance Access (entrance and exit)
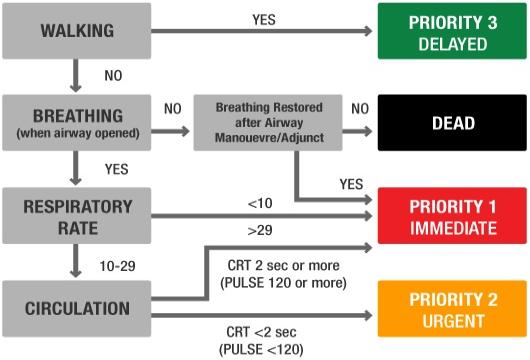
How are the patients Triaged in the field?
Triage
- A ”Sieve’ and ‘Sort’ approach is typically used by the team at the scene
- Walking patients typically receive the lowest priority (see below)
Team Priorities
- Triage
- Treatment (meaningful, resource appropriate)
- Transport

What are the Methods of Triage at the Scene?
Australian States use a Tag System:
Triage Tag

The Tag System allows a ‘Sieve’ and ‘Sort’ process to proceed rapidly at the scene of a disaster.
What are the Pros and Cons of a Tag System?
PROS |
CONS |
Documentation of Assessment |
Training |
Handover(effective compared to multiple verbal handovers in difficult environment in the field) |
DislodgementVital Signs May Change overtime |
StandardisedVariation Between StatesVisible – Basic Triage |
Ethics(Best Outcome for most rather than individual, no autonomy)‘Dying Patient’ Tagging (Expectant)Children (small) are all ‘non walking’ even if they are stable – higher priority (may also be a pro of tags) |
Interchangeable (single tag) |
Unfamiliarity |
Time Efficient |
Language |
Water Resistant |
Wet Conditions, Blood etc |
(1) ‘Dead’
(2) Critical
(3) Semi-urgent
(4) Walking
Specific Disaster Situations
(a) Bomb Blasts
- Primary – Related to the Blast Wave
- Secondary – Related to Shrapnel, Fragments, Debris from Blast
- Tertiary – Related to being thrown into wall etc from force (blunt chest, abdo and limb)
- Quaternary – Injuries related to Building Collapse, confinement, smoke inhalation etc.
(b) Chemical Agents
Nerve Agents |
Examples:Vx, Sarin, Taubin, Organophosphates |
Clinical:‘DUMBELS‘ (Cholinergic Effects such as Diarrhoea, Urination and Secretions) |
Treatment:Decontamination, Atropine, PPE, ‘oximes’, Supportive |
Blood Agents |
Examples:HCN CNCL |
Clinical:Lactic Acidosis |
Treatment:Sodium Thiosulphate, B12 |
Vesicants |
Examples:Mustard, Lewisite |
Clinical:Blistering, Cough, Airway |
Treatment:Chelating Agents, Supportive |
Respiratory Agents |
Examples:Chlorine, Phosgene |
Clinical:ARDS |
Treatment:Supportive |
(c) Pandemics and Infectious Diseases
The Middle Eastern Novel Coronovirus is the latest in a line of serious communicable infectious diseases.
Pandemics have the potential to overun Emergency Departments and the SARS outbreak of 2003 killed a number of medical staff who treated the patients…
The following factors are likely to be important to consider:
- Patient Factors
- Resuscitation, Isolation, Disposition, No NIV or Nebulisers
- Use of Rapid and Point of Care Testing
- Department Factors
- Isolation (see below), Briefing of Staff – Contact Public Health
- Modify Triage
- Containment of this Patient
- Signage
- Single Room
- Barrier Nursing
- No High Risk Staff Members (Pregnant) in Direct Contact
- N95 Mask, goggles, gown, PPE, terminal cleaning
- External Factors
- Media Interest
- Hospital Stakeholder Notification
- CEO, Media Liaison
- Preparedness for further patients
- Expect ‘worried well’ patients presenting to ED
- May need Protocols for these patients
- Check Stocks of Anti-viral Medications
- Consider ‘off site’ flu clinic
- Manage Staff Absences
- Prevention
- Immunisation Programs prior to Incident
- Staff in ED – Education and In-services, Disaster Preparedness
Summary
Overview (P.P.R.R.)
Prevention, Preparedness, Response and Recovery
Preparation (P.A.E.D.S.)
People, Area, Equipment, Department Resources and Send for Help (e.g. Notify Blood Bank, Theatre, Specialists and in this case Switchboard to activate the Disaster Plan)
Other Resources
Queensland Disaster Plan (2011)

Pretty nice post. I just stumbled upon your weblog and wanted to say that I’ve really enjoyed
browsing your blog posts. After all I will be subscribing
to your rss feed and I hope you write again soon!