
SYNCOPE PDF HANDOUT – CLICK HERE
Syncope in the Emergency Department (ED)
Introduction
Syncope is common accounting for about 1 in 50 of Emergency Department (ED) presentations. It is recurrent in 30% of patients and is characterised by a ‘Brief loss of consciousness that resolves without intervention’.
Syncope is derived from Greek “syn” – with and “koptein” to cut off or strike

In order to fit the definition of Syncope the episode has to be:
-
- Brief (no ‘set time’ but there should be no prolonged period of loss of consciousness or confusion)
- Transient (there needs to be a complete and spontaneous recovery)
Patients and bystanders may describe Syncope as a “blackout”, a “faint”, a “funny turn” or even a “seizure”.
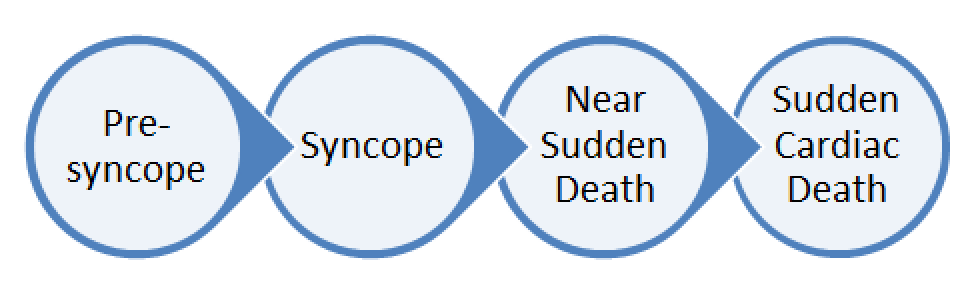
Key Concept – There is a ‘spectrum’ from pre syncope to syncope and from near-death to sudden death. The presentation of Syncope to the ED can be an opportunity to diagnose life-threatening underlying Cardiac Abnormalities. There are many high-profile cases of sudden cardiac death or ‘near misses’ such as the case of the footballer pictured below who had an undiagnosed malignant heart condition and suffered a Cardiac Arrest:

Common Diagnoses – Cardiac (Primary) 10-15%, Neurovascular 10-15%, Vasovagal 30%, Unknown Cause (Majority).
In true Syncope the important ‘rule out’ conditions to consider are generally “Cardiac” rather than Neurological. ‘Stroke’ and other neurological problems generally don’t cause true Syncope as defined above.
Pathogenesis of Syncope
Syncope is manifested by a short-lived period of Hypoperfusion which in turn leads to a loss of consciousness due to neurological dysfunction affecting the cerebral hemispheres and reticular activating system (RAS).
- Factors that maintain cerebral perfusion include:
-
- Cardiac output
- Systemic vascular resistance
- Mean arterial pressure
- Intravascular volume
- Cerebrovascular resistance with intrinsic auto-regulation
- Metabolic regulation
-
Diagnosis of Syncope
There is a vast list of potential causes of Syncope. A list of 50 causes is probably not really that helpful and would be difficult and impractical to memorise anyway. In the Emergency Department, it is probably most important to make a judicious assessment of the patient in order to rule in life threatening causes such as cardiac arrhythmia and rule syncope ‘mimics’ such as Seizures. The two key steps are confirming the patient indeed has true ‘Syncope’ (as per the definitions above) and if they do have Syncope, is there are underlying ‘commonly deadly’ diagnosis?
While an alternative diagnosis (CVA, TIA, Seizure) should be considered and looked for on neurological examination, they are unlikely to present with isolated syncope. Diagnosis of neurological disorders in the ED are usually made from other features of the presentation. Vascular Catastrophes such as Aortic Dissection may present with syncope and it is important to consider these in the assessment (see the “Rule of 15’s” below)
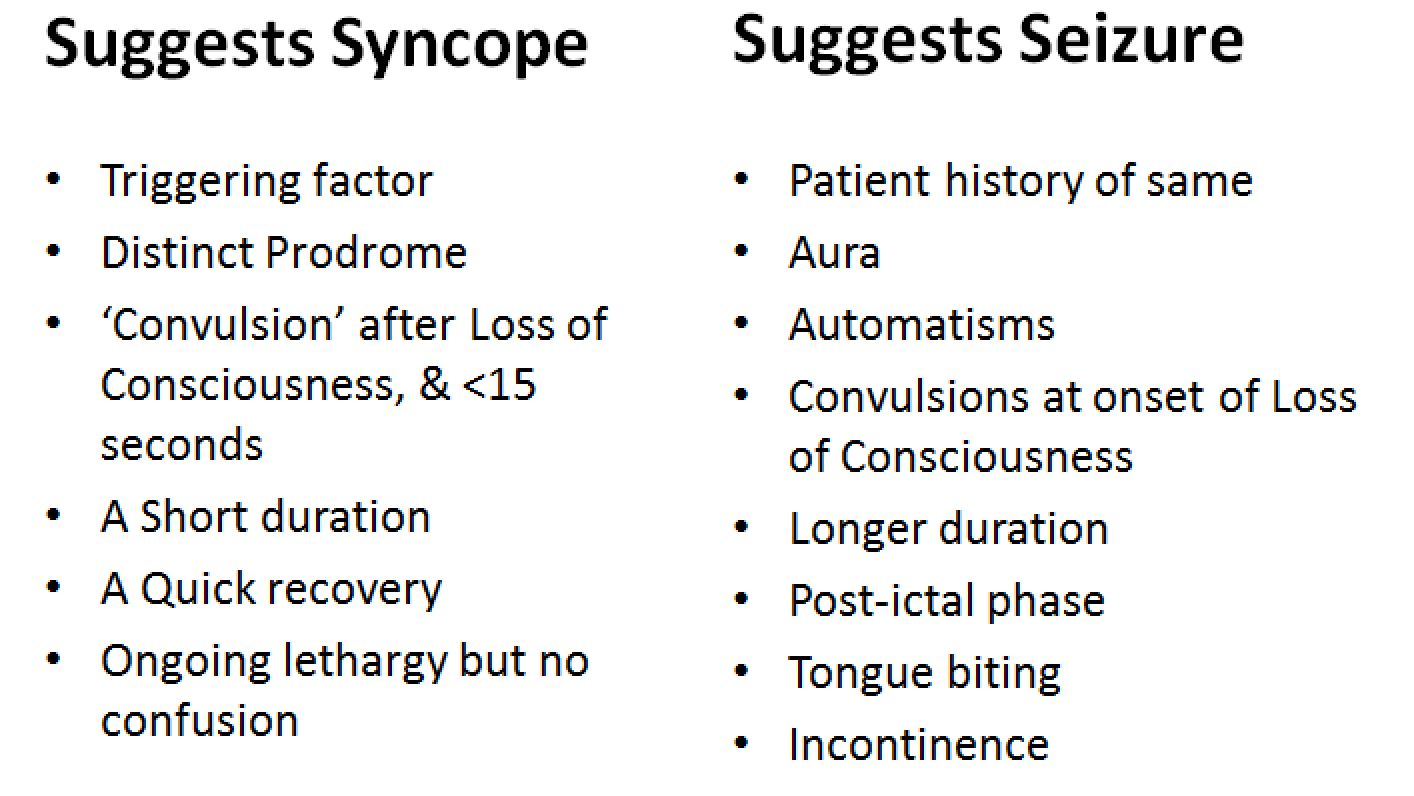
Question 1 – Does the patient have Syncope or Seizure?
Question 2 – What are the Goals in the Assessment of Syncope?
4 Steps in the Evaluation in the Emergency Department
- Step 1 – Distinguish Syncope vs Seizure (see above)
- Step 2 – Make a Diagnosis
-
- The majority of patients will be diagnosed in the ED rather than on the wards
- Consider the ‘Rule of 15‘ – (e.g. 15% of patients with these disorders present with ‘Syncope’)
- Many Investigations may be appropriate but should be targeted at the patient presentation
- The ECG should be considered an “essential” investigation in all patients with Syncope (our ECG page is available here and we discuss the specific ECG patterns to look for later on in this article)
-
- Step 3 – Risk Stratify the undifferentiated patient
-
- Use Clinical Judgement
- Use Decision Rules as a common sense ‘checklist’
- Decide if the patient has any “high risk” features or is “low risk” based on the ED assessment
-
- Step 4 – Refer and Admit high risk and ‘red flag’ cases appropriately
The Rule of 15’s

Question 3 – What are the options for evidence based decision-making?
- Decision Rules and Clinical Policies have been widely used in the evaluation of Syncope.
- Clinical Rules are useful for the following:
- As a Checklist – a ‘check-listing’ of your own assessment of the Syncope patient
- Educating junior doctors and medical students about the key features of a syncope assessment
- For documentation of the Emergency evaluation in a structured manner
- The Disadvantage of Clinical Decision Rules are that may rules can be oversimplified or very broad (i.e. they may be under or overly sensitive). They are unlikely to be as accurate as an experienced medical practitioner especially in complex presentations such as Syncope. The rules described below are best used to support clinical decision-making and documentation as described above
Syncope Rules
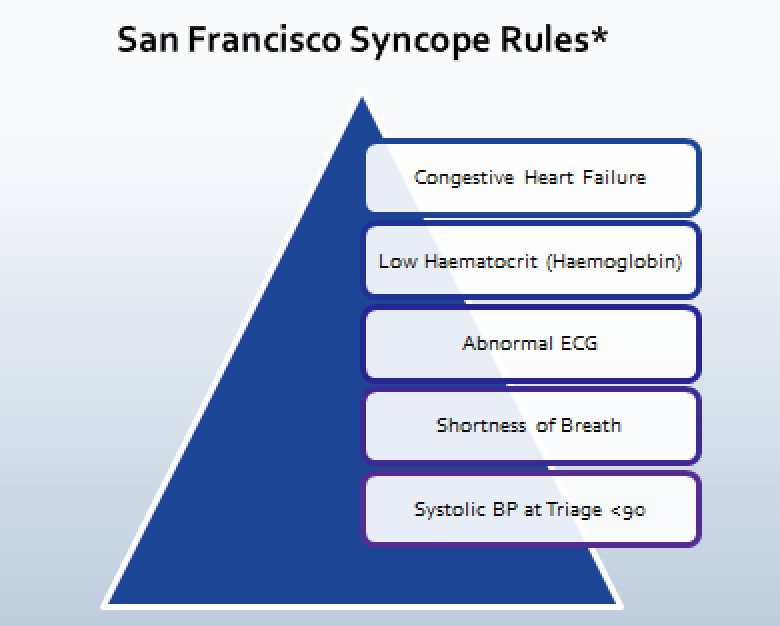
(1) San Fransciso Rules*
- Predicts “higher likelihood” of 30 day adverse outcome
- Also known as the ‘CHESS’ Criteria
- Pros – Simple, Memorable, Teachable
- Cons – Limited External Validation – may miss (rare) high-risk diagnosis
(2) Boston Syncope Rules**
- Rule out Criteria – prospective outcomes were evaluated at 30 day follow-up
- Pros – Detailed, Comprehensive, Evidence Based
- Cons – Complicated – the figure below shows the 8 major domains included (there were 25 in total)

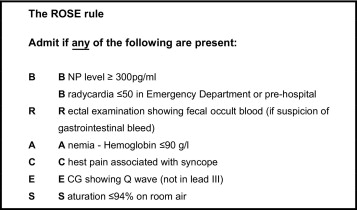
(3) ROSE Criteria (BRACES Rules)
- Prospective Cohort Study of Syncope patients – 1 month follow-up
- Pros – Simple, Memorable
- Cons – This score uses BNP (expensive and not available easily at many hospitals in Australia)
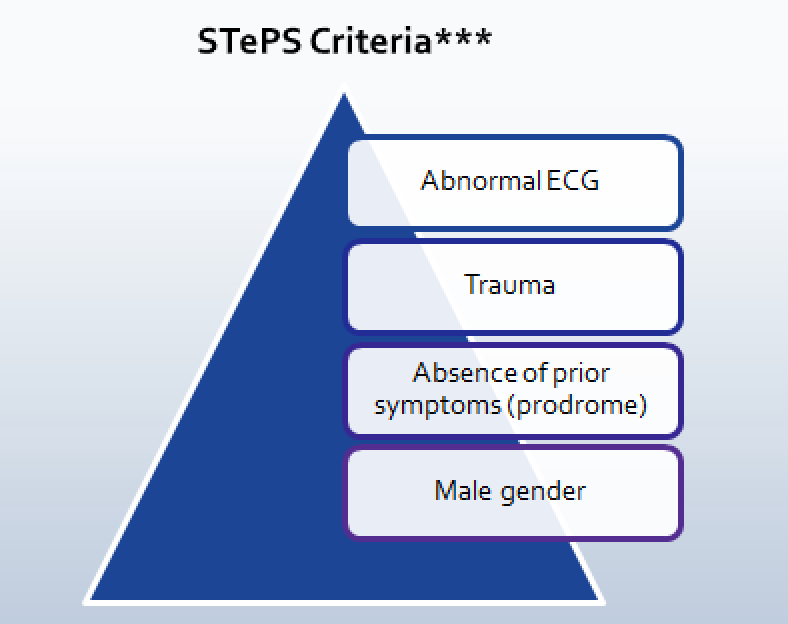
(4) Short-Term Prognosis of Syncope (STePS) ***
- Predicts patients for risk of “severe adverse outcomes” at 10 days
- Pros – considers both short and long-term outcomes
- Cons – delayed evaluation and publication
Question 4 – What are the high risk features associated with Syncope?
- Red Flags in the History
- Old Age
- Cardiac Disease
- Syncope on exertion
- Syncope while lying down (recumbent)
- Family History (Sudden Death)
- Positional Symptoms (may be more reliable than Orthostatic Blood Pressure and Heart Rate)
- Recurrent Syncope
- Prolonged Loss of Consciousness
- Medications that affect cardiac conduction
- Examination Key Steps
- Cardiac Exam
- Blood Pressure
- Pulse
- Murmurs
- Abdominal Exam
- Ectopic Pregnancy
- AAA
- PR exam and Faecal Occult Blood (FOB) Testing
- Neurological exam
- Cranial Nerves
- Limbs
- Cerebellum
- Cardiac Exam
- Investigations
- ECG
- Should be done in all patients
- Full blood count
- Especially in older patients
- Blood Sugar Level
- ECG
-
- Non-routine tests – should be used selectively
- Specific Blood Tests
- Orthostatic BP – generally not specific or sensitive – probably overused in the ED
- Holter Monitoring – may not add much to a ‘normal ECG’
- CT head – has a low yield when used non-selectively
- USS Doppler
- Echocardiography
- Non-routine tests – should be used selectively
Question 5 – What are the key diagnoses to exclude on the ECG?
- Acute Coronary Syndromes
-
-
- STEMI, NSTEMI and Unstable Angina
-
-
- ECG Changes associated with Pulmonary Embolism
-
-
- T wave inversion and RV Strain Pattern
- Sinus Tachycardia
- S1 Q3 T3
-
-
- Slow Arrhythmia (look for bradycardia and heart blocks)

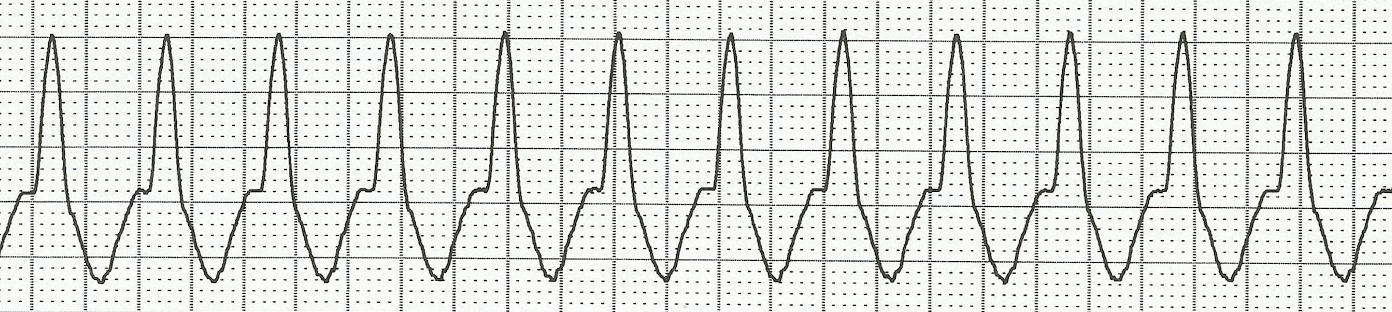
- Fast Arrhythmia – (look for tachycardia – broad and narrow complex)
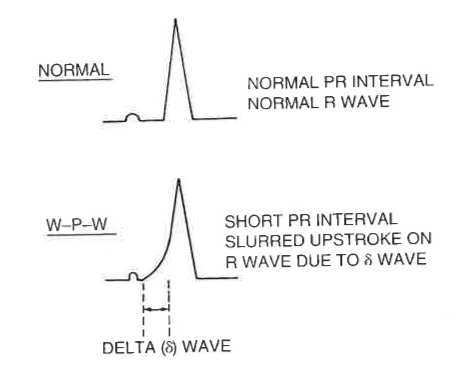
- Wolf Parkinson White
- Pre-excitation (Delta Waves)
- Brugada Syndrome

-
- Brugada Type 1 – Elevated ST segment (>2mm) descends then has upward convexity + T wave inversion
- Brugada Type 2 – Elevated ST segment (>1mm) descends toward baseline then rises to upright T wave
- Brugada Type 3 – Elevated ST segment (<1mm) descends toward baseline then rises to upright T wave
- Arrhythmogenic RV dysplasia (ARVD)
-
-
-
- The Classic finding in this rare condition is ‘Epsilon Waves’
-
-
-
- Cardiomyopathy (e.g. Hypertrophic Cardiomyopathy – HOCM) – classic mimic of Aortic Stenosis (similar murmur) causes outflow obstruction – 50% have family hx
- QT Prolongation
- QT Shortening – RARE but can cause Syncope and Arrythmias
- Toxicology (e.g. Sodium Channel Blockade such as Tricyclic Overdose)

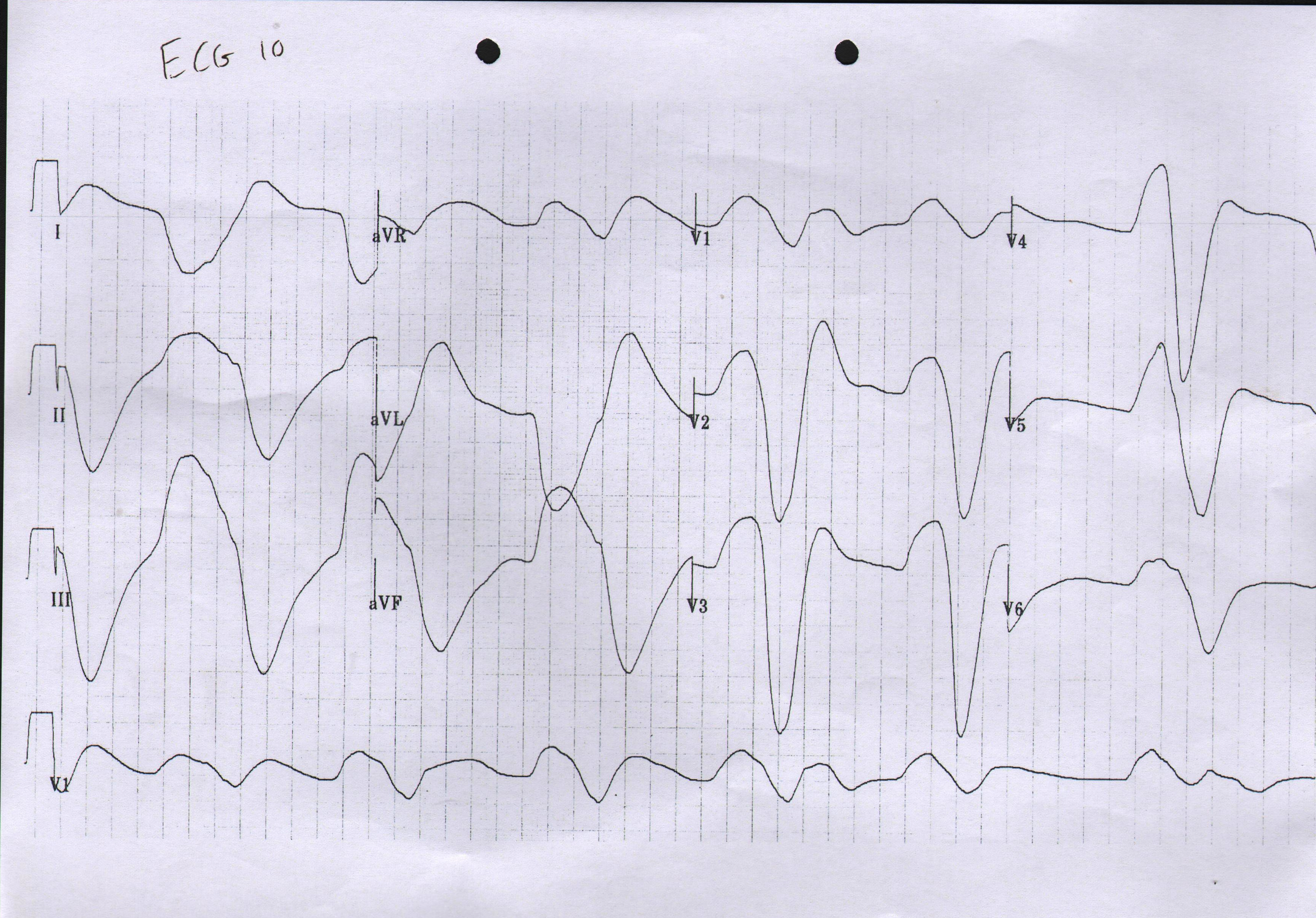
- Electrolytes (e.g. Hyperkalaemia)
Summary
It is important to understand the definition of syncope (including brevity, loss of consciousness and postural tone with spontaneous recovery) as well as associated high-risk features.
It is also important to develop skills in differentiating Syncope from other presentations such as vertigo and seizures. Admission to hospital is often required in patients with Syncope but does not always help make a definitive diagnosis. Where in doubt, share the case with a colleague, use a clinical decision rule and choose appropriate investigations to help risk stratify the patient and rule out life threatening causes.
Links to Further Reading on Syncope in the Emergency Department
- Syncope LITFL – Click Here
- EM Ireland Syncope – Click Here
- SEMEP – Click Here

This review by Reed et al from 2006 is a good Emergency Based overview – http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2564156/