
(5 Minute Read)
eCPR
Extracorporeal cardiopulmonary resuscitation (eCPR) uses veno-arterial extracorporeal membrane oxygenation (VA-ECMO) to provide circulatory support during selected cases of refractory cardiac arrest.
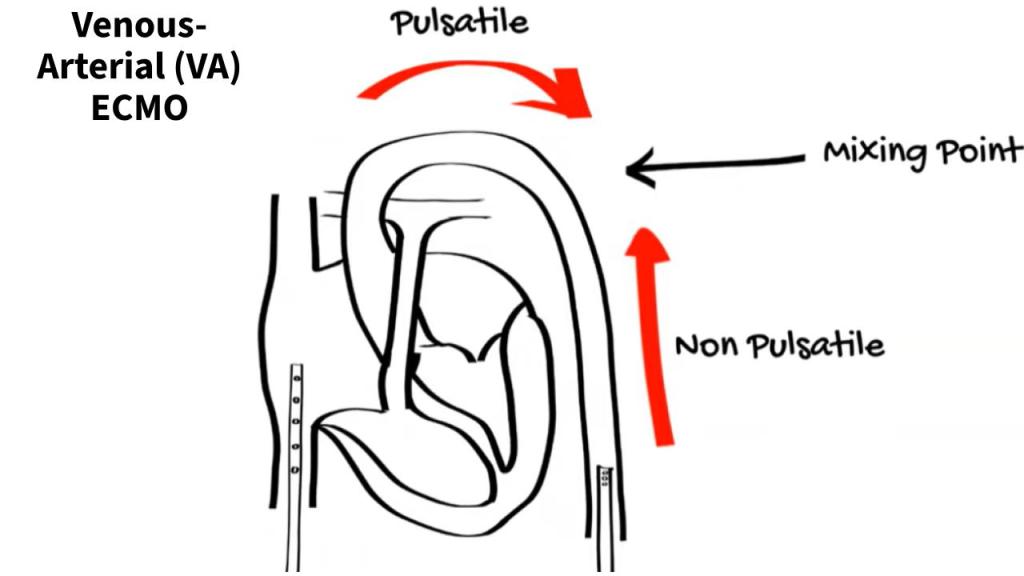
The technical challenge is obvious: vascular access, cannulation, circuit preparation and time-critical decision-making must occur while high-quality resuscitation continues.
Non-technical Skills
But eCPR is not simply a cannulation procedure.
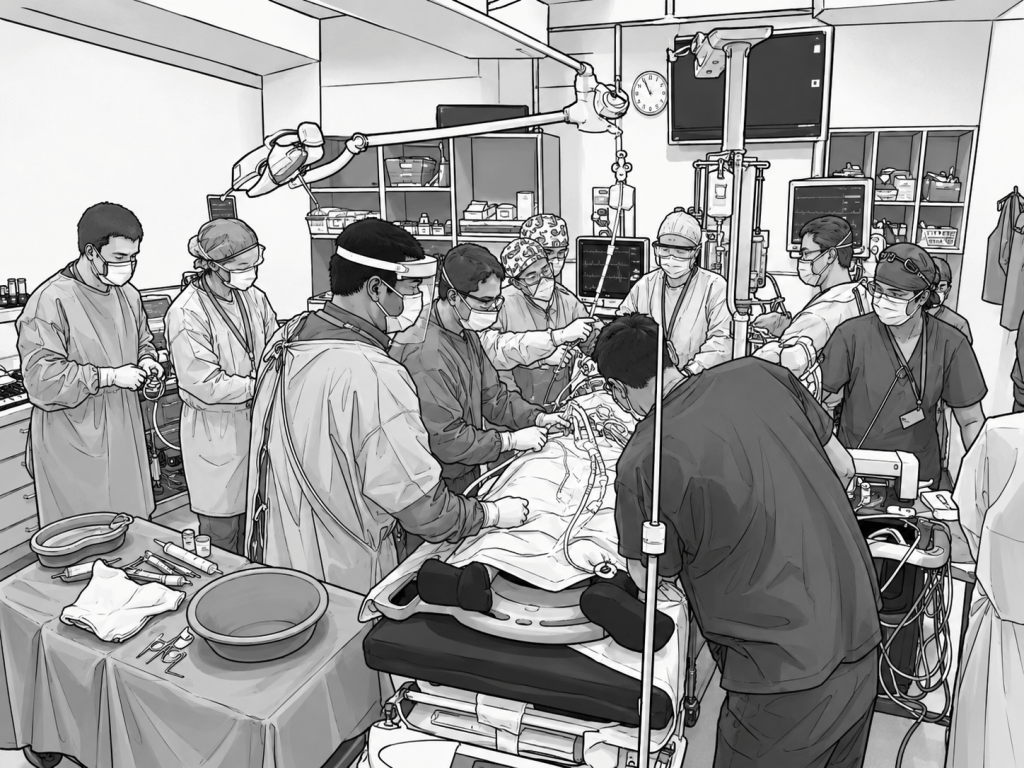
It is a high-acuity, low-occurrence event with a substantial coordination and environmental burden.
Large interdisciplinary teams assemble rapidly, often involving clinicians who may not routinely work together. Noise, crowding, competing conversations, equipment movement and changing clinical priorities all shape performance.
Talking at the SESAM Conference this week I focussed on the Human Factors elements in eCPR from a recently accepted study from our team in Sydney.
NB – For those interested in the technical bits we have a free Smart Phone app describing eCPR and ECMO:

Pilot Study
Back to the human factors issues in implementing eCPR…
In the small exploratory study (recently accepted at BMC Emergency Medicine) we examined human factors. In the first phase there was an inital in pilot simulation study. Once the methods weer refined we targetted real emergency department eCPR events…
Before observing the clinical eCPR cases, we used in situ simulation to rehearse the research itself.
Simulation allowed us to test data sheets, observer positioning, physiological monitoring and workflow.
It also showed us what was impractical: video tracking and pedometers were abandoned, while teamwork observation, noise measurement and selected stress measures were retained.
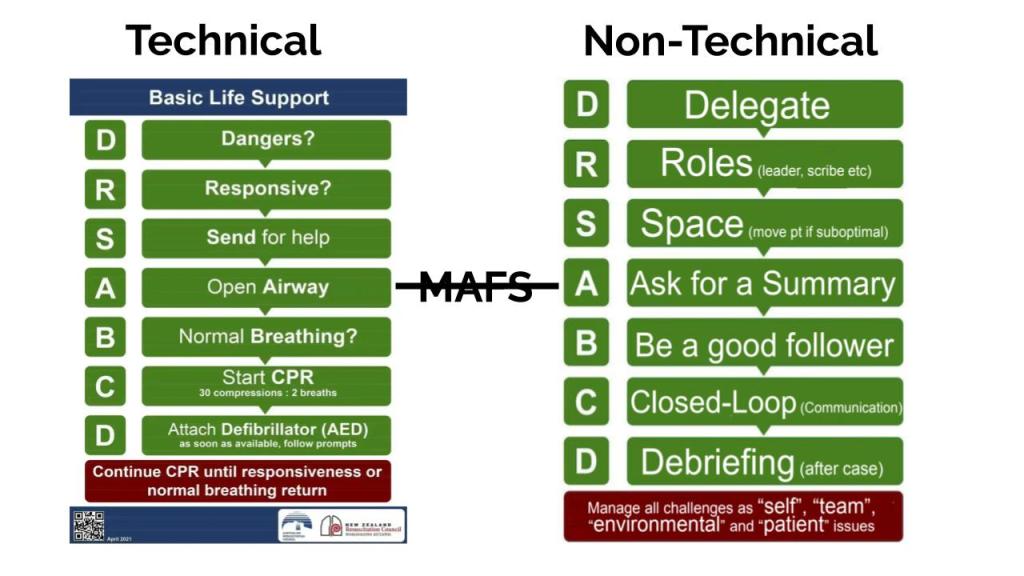
Cliff Reid’s work on Teamwork and Human Factors was a big influence in the planning of the study:
eCPR Study
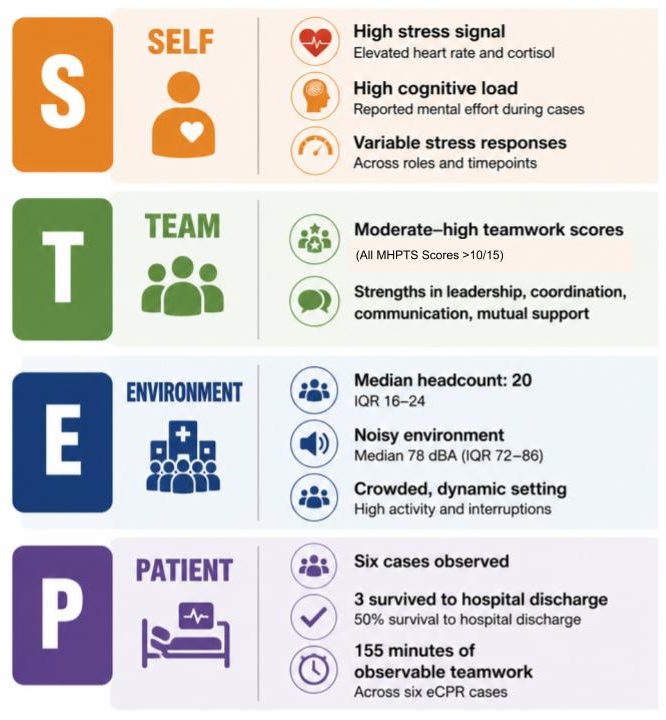
Across six eCPR events, 18 clinicians were observed. Teamwork scores were generally moderate to high, with a median Mayo High Performance Teamwork Score of 12/15.
However, the environment was consistently demanding: the median room headcount was typically >20, with some cases involving considerably more people.
Stress signals apparent, and salivary cortisol measurements higher after eCPR than in paired baseline samples. Noise and crowding were prominent features of the clinical environment.
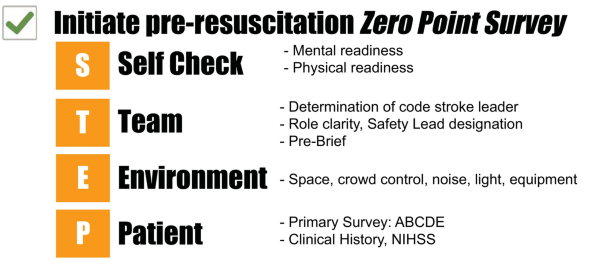
Several system-level practices were repeatedly observed in the study should be noted:
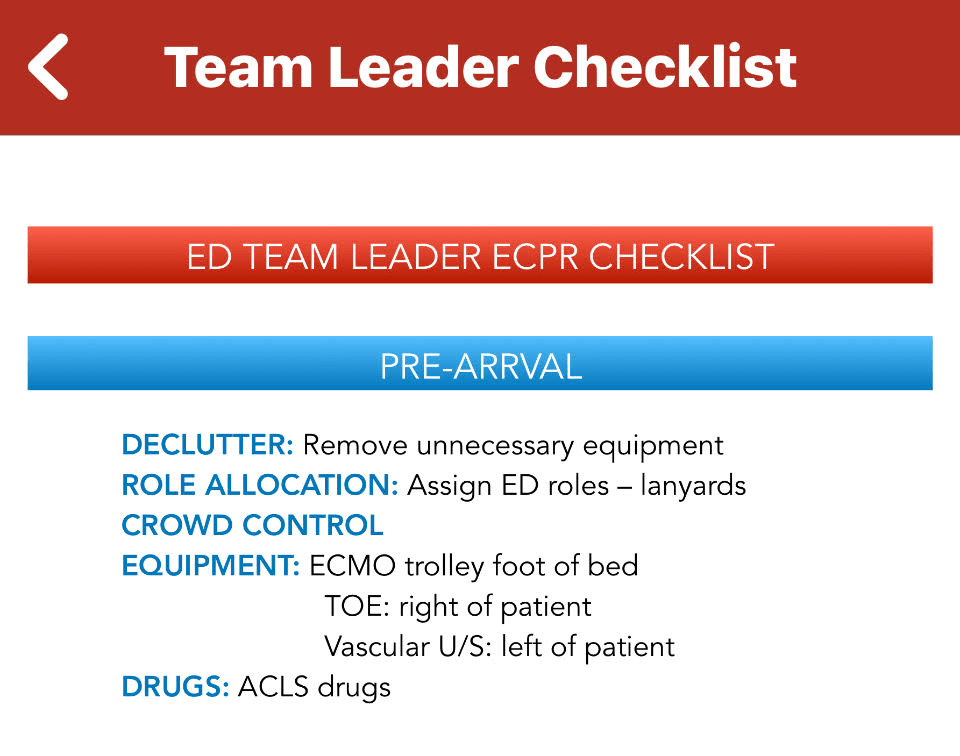
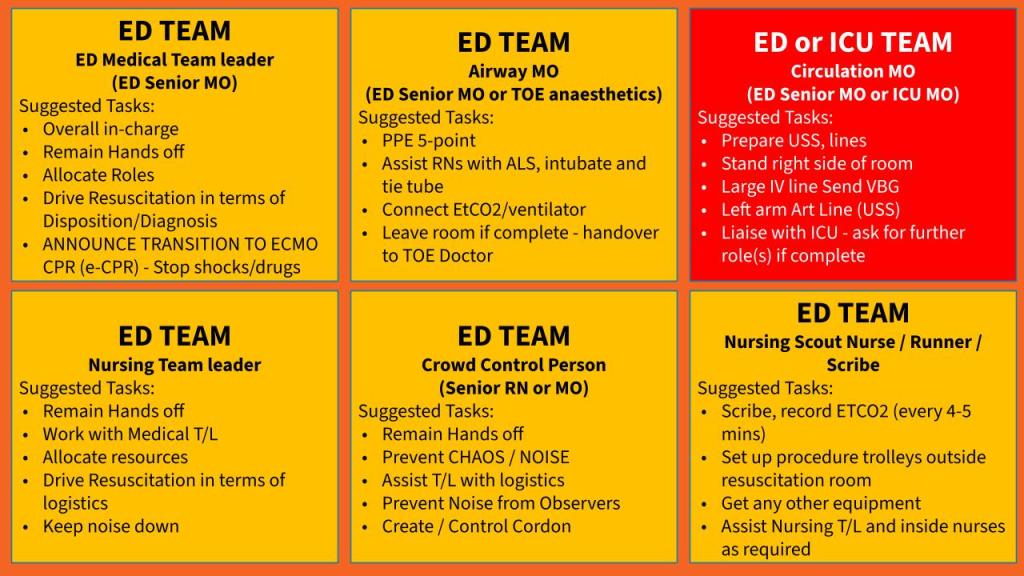
Predefined roles (Pictured)
Controlling the Spaces (with Lanyard Passes and a Physical Cordon)
Designated crowd-control leadership and structured team-leader summaries based on checklists (Pictured).
eCPR Human Factors
The lesson is straightforward. eCPR training should not focus just on technical proficiency with inserting cannulas or operating the ECMO circuit.
Training for eCPR teams should reproduce the elements of the system around the procedure: crowding, noise, role allocation, handovers, communication degradation, uncertainty and transitions in leadership.
Simulation’s Role
In this study, simulation supported eCPR in three distinct but connected ways.
- Simulation helped design the clinical system itself. Repeated in situ simulations allowed the team to test role allocation, room layout, equipment positioning, communication pathways, crowd control and transitions from conventional resuscitation to eCPR. This moved simulation beyond individual technical training and into system design. Moreover, simulation was a key to success in our view. It helped us practice (cannulation) and after real cases we learned from the few actual High Acuity Low Occurence (HALO) cases when they came in…
- Simulation was used as a research rehearsal tool. Before attempting data collection during rare real-world events, the investigators tested observer positioning, monitoring equipment, teamwork scoring, noise measurement and follow-up processes. Some planned measures, including video tracking and pedometers, proved impractical and were removed.
- Simulation provided a bridge back from observation to improvement. Findings from actual eCPR cases (including crowding, noise, communication demands and variable stress responses) could be translated into future scenarios, team briefings and debriefing processes.
For eCPR and other HALO events, simulation is not merely preparation for the procedure. It is a method for testing and strengthening the entire system around it.
Simulation therefore can become the glue in a continuous cycle: design the system, rehearse the research, observe real performance, identify vulnerabilities and then return to simulation to test possible improvements.
Take-Home
For eCPR (and other HALO situations) we need to train the system—not just the cannulation
