


Video Lecture (10 minutes)
Background
Debriefing in the Emergency Department of “real-life” cases is a current topic of interest and controversy in the medical education community.
Facilitated discussion following a meaningful clinical experience has the potential to enhance learning, improve team culture, provide substrate for quality improvement initiatives and identify latent patient safety threats.
However, single session “forced” debriefing in other contexts has also been associated with increased distress and post traumatic stress disorder (PTSD). This has put a limitation on progress in this area since 2002, though it should be noted most of these debriefings were for individual patients rather than communities of hospital-based teams. In our opinion, while the benefits are likely to outweigh the risks one should be mindful of the tension of needing to focus on emotional issues versus learning.
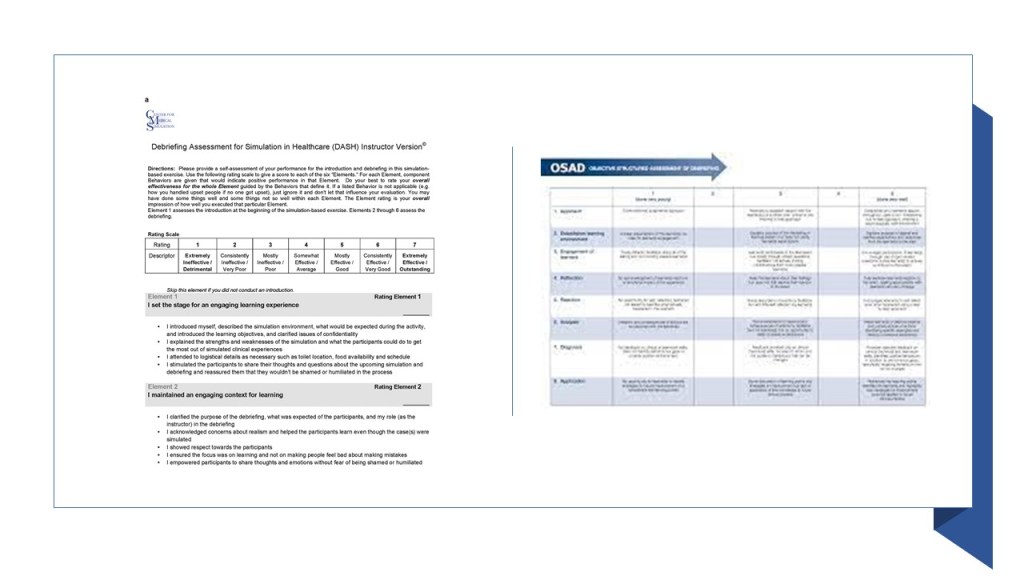
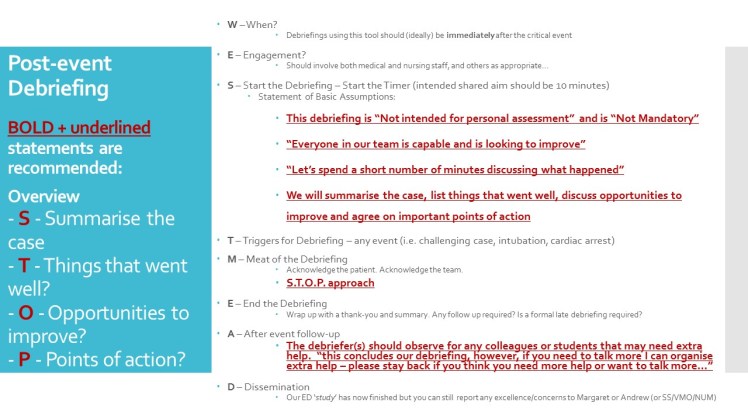
The opportunity for learning team based cognitive, procedural and behaviour skills in this context is fairly obvious, but just like in Simulation Based Medical Education we must maintain psychological safety for all the members of the team. On this page we share our local rubric for debriefing based on the INFO tool (Calgary) and STOP tool (Edinburgh) all of which could be a basis for your local program:
The STOP tool
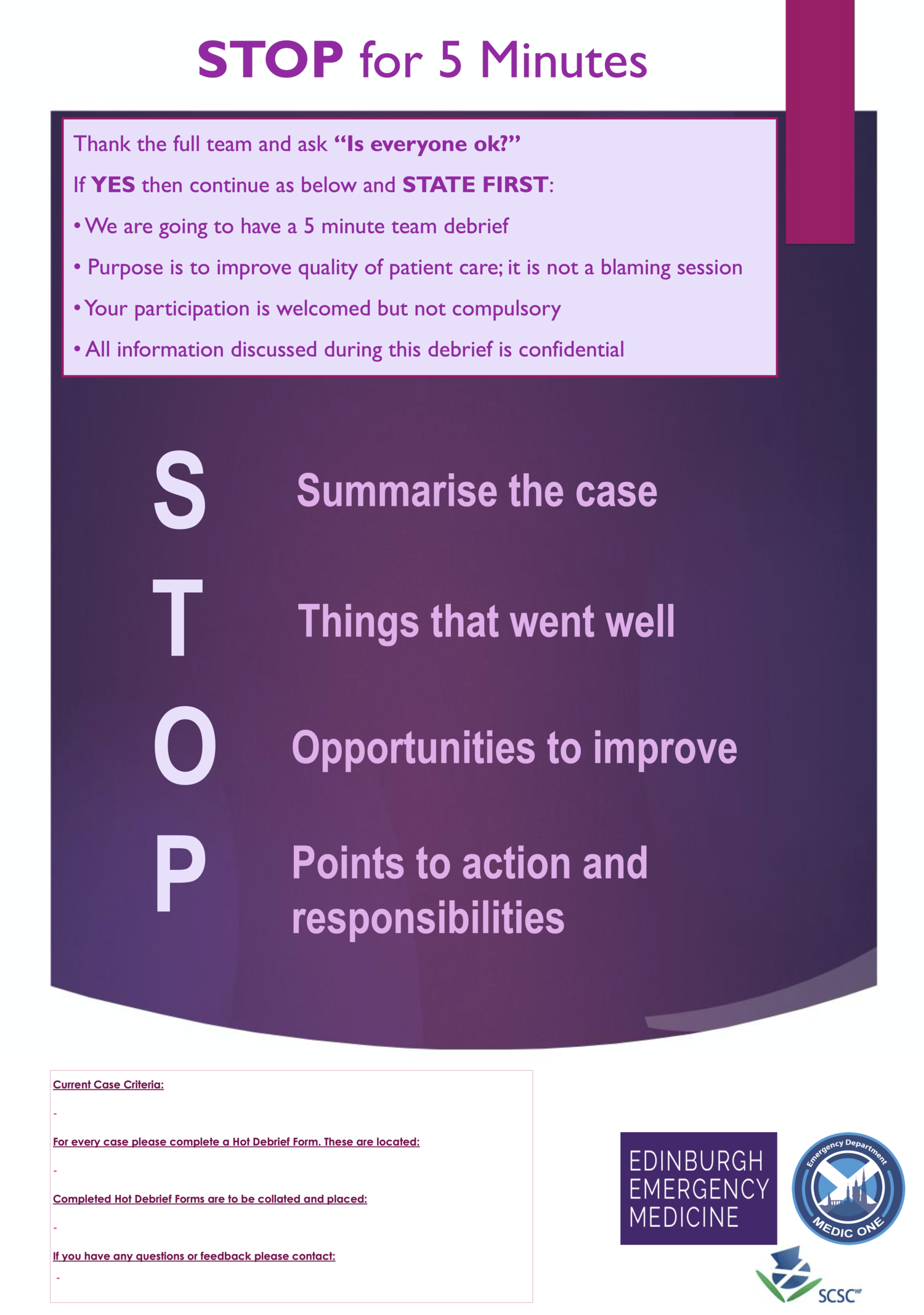
Click Link Here
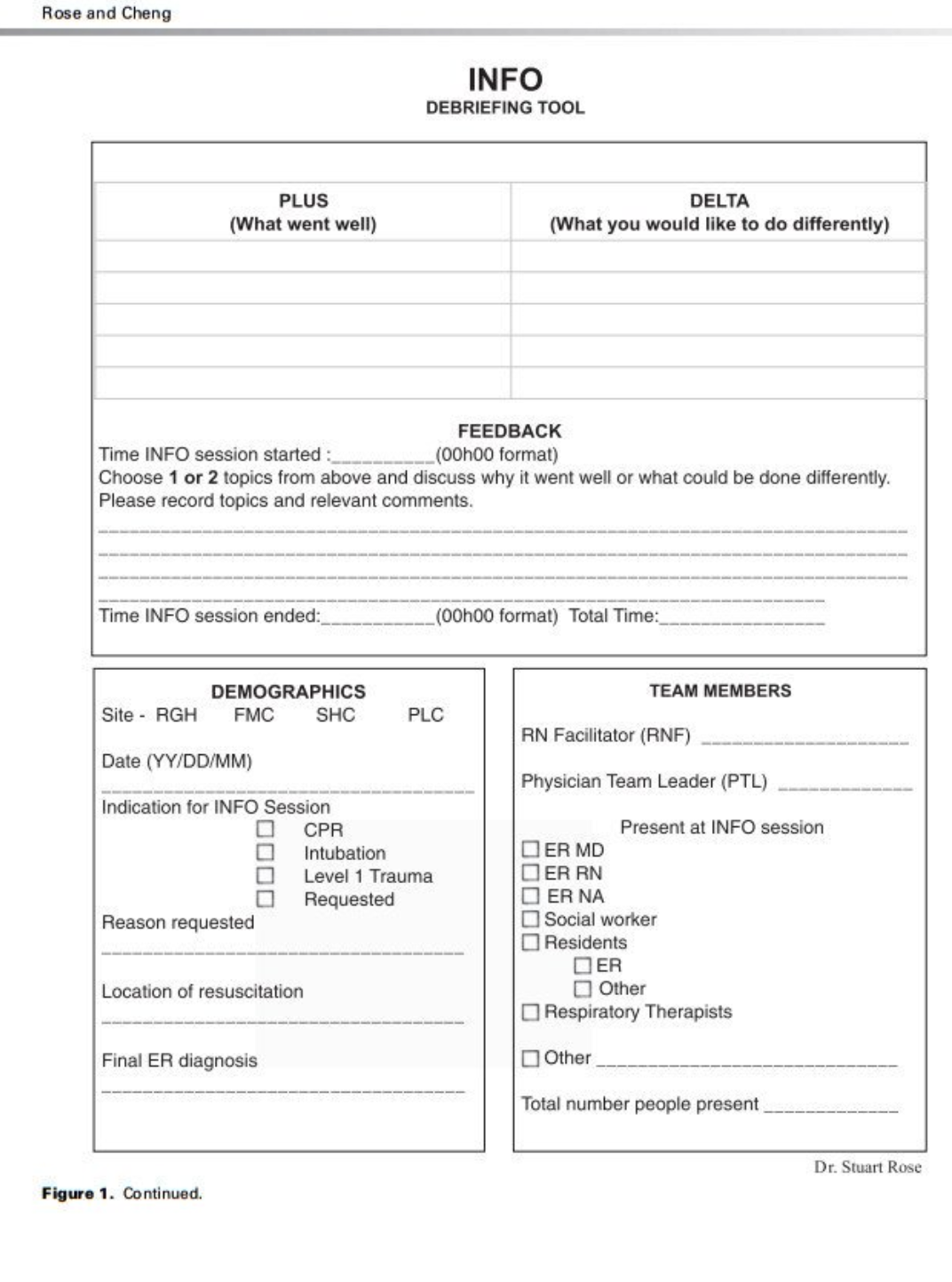
The INFO tool

A Blended Tool for our Emergency Department
Our Audit of ED Practice
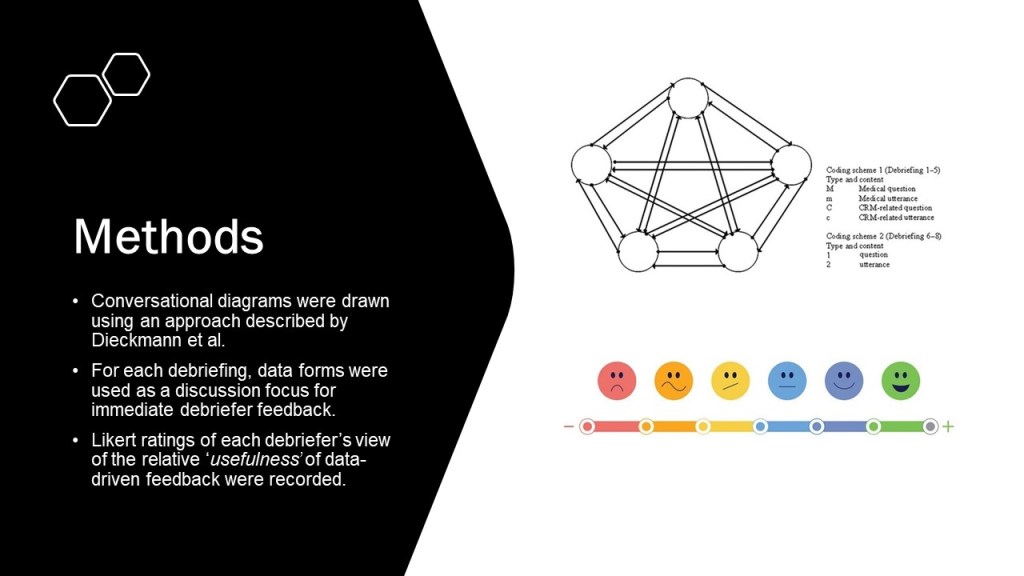
During our recent audit of our local tool based on the INFO and STOP models we observed >50 debriefings. As a result we mapped the discussion content (domains) used during Clinical Event Debriefing.
Reassuringly, the typical topics (PEARLS domains) from simulated cases also come up in clinical debriefing. They accounted for around 80% of conversation in our audit of practice. This means you should feel confident as an educator that you have some of the baseline skills required to debrief cases that are not highly distressing.
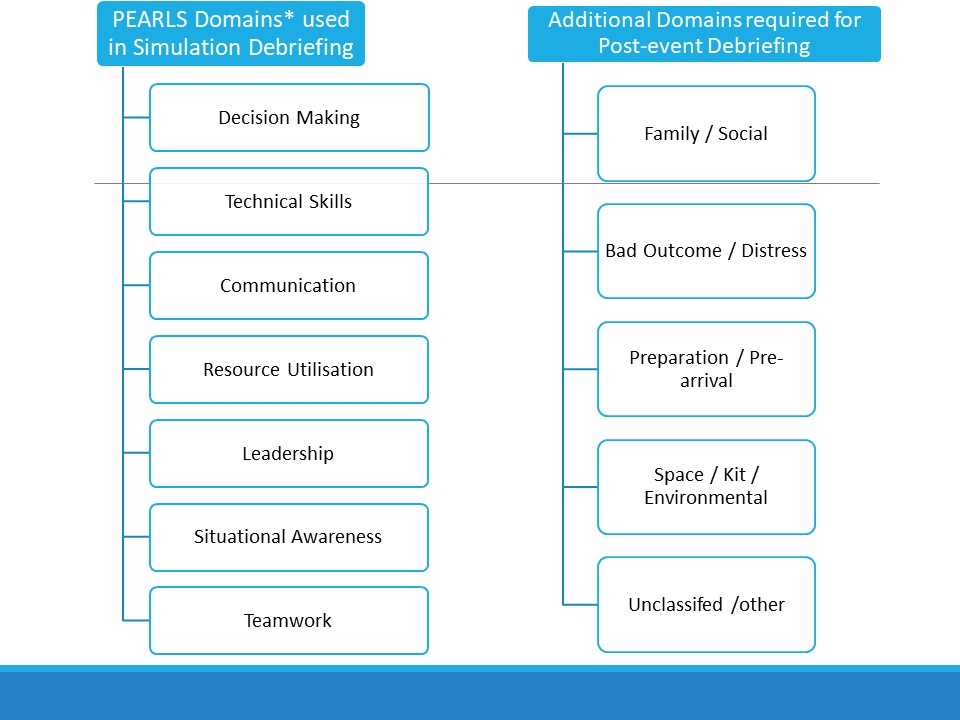 *Promoting Excellence and Reflective Learning in Simulation (PEARLS)
*Promoting Excellence and Reflective Learning in Simulation (PEARLS)
An example of an airway case that was debriefed in our ED (with permission):

Some clinicians believe that clinical debriefing should be limited to cardiac arrest cases and “bad outcome” situations. However, our local experience is that rich learning for individuals, teams and systems can come from many other types of case. Indeed, in our audit debriefings typically took 10 minutes, involved on average 7 people and were led by both nurses and doctors…
Many questions remain on this topic including:
- how much training do facilitators need?
- what should that training look like?
- should the debriefer be external to the event or can it be someone involved in the case itself?
- are there medicolegal implications of recording details of the event if (it is not anonymised)?
- how do we measure the effectiveness of this type of debriefing?
- should we use cases as substrate for clinical governance and in situ sim
- if so how soon is too soon (sim) and how much should be reported (governance)?
Case types included in Debriefings:
| Clinical Events | Number of Debriefings |
| Major Trauma (n/%) | 12 |
| Airway (n/%) | 8 |
| Cardiac Arrest (n/%) | 19 |
| Psychiatric Emergency (n/%) | 1 |
| Medical Emergency (n/%) | 10 |
| Surgical Emergency (n/%) | 1 |
| Thoracotomy (n/%) | 1 |
| Obstetric (n/%) | 1 |
| TOTAL | 53 |
Well-being of Staff
Westmead Specific Plan and Contact Numbers
- Exposure to potentially traumatic events such as cardiac arrest resuscitation, traumatic motor vehicle collisions, catastrophic injuries, disaster responses, as well as extraordinary tragic circumstances, can have significant impacts on the overall wellbeing of staff.
- Vicarious trauma is easily overseen, when we are busy attending to the needs of patients and families in a busy and demanding work environment.
- Generally, emergency department staff have a high sense of resilience, however the cumulative effects of experiencing these unavoidable events can have significant impacts on our emotional and psychological health. Staff are encouraged to seek help as required, continue to maintain a good culture of offering each other support, and engage in good self-care practices.
Below are some helpful contact numbers and resources for you to access:
Local Plan – CLICK HERE
- Employee Assistance Program (1800 81 87 28) for individual phone or face to face counselling
- GP Mental Health Plan – referral for counselling
- Men’s Line Australia (1300 78 99 78) https://mensline.org.au – phone and online counselling
- Cumberland Women’s Health Centre, Harris Park (9689 3044) http://www.cwhc.org.au – counselling and support focussed on the health and wellbeing of women (means tested)
- Beyond Blue https://www.beyondblue.org.au
- Black Dog Institute https://www.blackdoginstitute.org.au
- Phoenix Australia https://www.phoenixaustralia.org
- Headspace App
- EAP in focus App
- TREAT App
- Smiling Mind App
Summary
Post-event debriefing of real cases appears to be a feasible and useful inter-professional educational activity in an ED setting.
Clinical debriefing is an emerging skill for hospital based clinical educators as well as the wider simulated based medical education community who may be asked to provide their skills in a clinical setting.
In our experience, using a simple approach to these debriefings can lead to meaningful team learning without an obvious risk of harm. ED staff, to simply do their job of working in the resuscitation bay, exhibit high levels of resilience and are unlikely to be harmed by this activity as long as trained educators conduct the debriefing and there is access to resources for individuals requiring extra support.
