A Classic LP Case
The Fictionalised Case (with permission)
A 45 year old gentleman presents to the Emergency Department (ED) by car with an on-going severe headache. The headache started 5 days ago.
The headaches were precipitated by sneezing whilst bracing a recently injured knee (diagnosed on MRI as a meniscal tear).
The patient reported ‘the worst headache of his life’, ‘maximal onset within seconds’. There was some transient improvement after retiring to bed and turning all the lights off.
After a fluctuating course for 5 days, the headache remained. He came to the ED with his wife – understandably they were both concerned about the cause of this headache.
From this history the ED team were concerned about Subarachnoid Haemorrhage (SAH). A CT head scan was requested and was analgesia provided.

A non-contrast CT scan was performed and reported promptly as ‘normal’:

Source – https://radiopaedia.org/cases/normal-ct-brain
After a short period of discussion and deliberation at the bedside we elected to perform a Lumbar Puncture (LP) to exclude SAH.
I have done (literally) scores of LPs for SAH and have recently read you would have to do several 100 to find one SAH (Sayer et al 2015). Doing a lot of low yield LPs is frustrating. However, the aim is to ‘never miss’ SAH because of the risk of ‘re-bleeding’ and ‘death’. Therefore, we preceded with LP in this case (with the expectation that the cause of the headache was still more than likely to be benign in view of the normal CT head).
High Risk Patients
In the event of a typical SAH story we would certainly advocate for doing a LP. An example of a ‘high risk patient’ would include if all of the factors on the ‘Ontario score’ are met or if there other concerns in the history such as a known aneurysm, polycystic kidney disease or family history. In this scenario, in the event that the LP is unsuccessful a CT angiogram could be used to look for an aneurysm with a referral to neurosurgical colleagues for a final patient plan.
In the case described, I felt the story was ‘high risk’. So, despite patient concerns about the idea of a spinal tap, we were able to do the LP (painlessly) in the end. This was aided by judicious dosing of ‘anxio-lysis’ (titrated IV midazolam).
Here is the appearance of the Lumbar Puncture:

Here are the LP results:
At the time I thought the LP was relatively non-traumatic, although we were successful on the second pass. We used a blunt bevelled needle (9cm) with a sharp skin introducer needle. The opening pressure was 29cmH2O.
As a result, we were alarmed. Could this represent SAH rather than a traumatic tap? Due to the appearances shown we quickly requested a CT scan with contrast while awaiting the LP results.
The new CT scan showed a moderate sized anterior communicating artery (ACOM) aneurysm – presumably the source of a bleed 5 days ago – and the patient was started on Nimodipine (given the possible risk of vasospasm).
At this stage the organisation of transfer to the local neurosurgical centre by air (some 300km away) was expedited and the patient was safely transferred with a good outcome.
Our Reflection Questions from this case
- How can we tell the difference between a Traumatic Tap and the rare ‘true’ case of Subarachnoid Haemorrhage?
- Is it really as safe practice to rule out with a CT alone?
- When the history is this ‘classic’ should we just do a CT with contrast?
- Are there any scores available to help us make good plans for our patients?
(1) Traumatic LP v SAH
Given the history given by the patient of symptoms typical of SAH, I did not think this was a “traumatic tap” – but how can you be sure? A study by Gorchynski et al (2007) provides a useful table of the typical numbers you should expect in LP with SAH versus LP with inadvertent trauma from the needle:
| Table 1 | Traumatic LP (n=142)
|
SAH (n=11)
|
| Tube 1 – Mean RBCs
|
6763 red cells
(95% CI 4029–9496)
|
399,277 red cells
|
| Tube 4 – Mean RBCs
|
443 red cells
(95% CI 295–592)
|
307,700 red cells
|
| Mean Percent
Change
|
-82.1%
(95% CI +84.9 to 79.9)
|
−9.1%
(95% CI-19.3 to 2.1)
|

Comparing the numbers in Table 1 to the case presented above would support a diagnosis of SAH in our case…
Another rule of thumb comes from another paper by Perry et al (2015). From Table 2 (shown below) my take home is if there is lots of red cells get more help (i.e. Neurosurgery) regardless. In these rare cases it is important to share decision making…
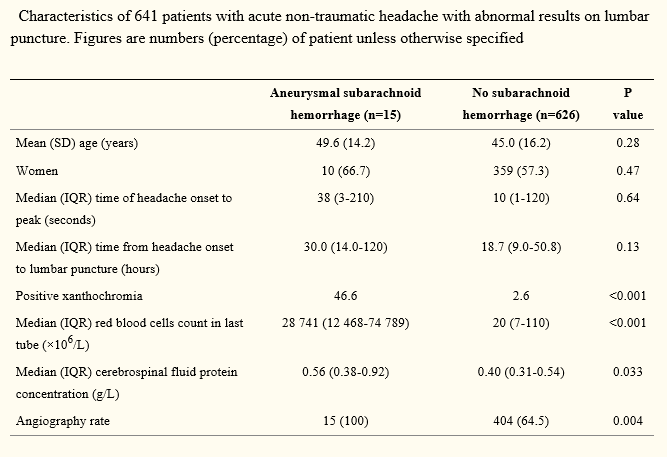
(2) Deferring the CT in low risk patients
Recently, following the landmark paper by Perry et al (2011), many advocate (controversially) deferring LP. Specifically this may be safe when the CT is reported in the first 6 hours of headache onset, and it is reported reliably by a radiologist.
Personally, I go on gestalt re this matter. Twitter polls of current practice suggest a range of practice in this situation. In my opinion, if the ‘post test probability’ is low AND you have an early negative CT AND only a vague story to fit SAH you can probably get away with not the LP. However, I am in the habit of always discussing (and documenting). The aim is to make a shared plan with the patient about the pros of deferring the LP.
Blok et al (2015) reported ZERO cases of death or negative outcomes in patients presenting with sudden onset of headache and a negative head CT performed within 6 hours or less of symptom onset of headache. This was an observational multi-site retrospective Study at 11 Non-Academic Hospitals with 760 patients. My take is the practice is probably ok, but a key step is a skilful explanation to the patient and document of their input in the final plan.
(3) Should we just do a CT with contrast?
This is probably not answerable in a short post. It seems that local practice takes precedence. If you do a CT with contrast you may find an aneurysm but you won’t know if it has bled without LP and you won’t know whether it will every bleed in the future without omnipotent powers. These two videos may help with the referral process:
(4) Are there any scores available that might help?
The SAH Ottawa score was recently validated in a paper in JAMA (again by the prolific SAH author Dr Perry):

