
Brief Case Study
- 33 year old female presented post Motorbike Accident (MBA)
- Our patient had been riding on a dirt trail when she lost control of the bike
- She was wearing a helmet and protective gear.

Primary Survey and Initial Imaging
- Airway Assessment – patent, patient was talking and orientated
- Breathing Assessment
- Palpation – normal
- Symmetrical Air Entry
- O2 sats of 98%
- Circualtion Assessment
- Blood Pressure of 135/70 and Pulse Rate of 88
- Disability Assessment
- GCS 15
- Blood Sugar 6.3mmol/L
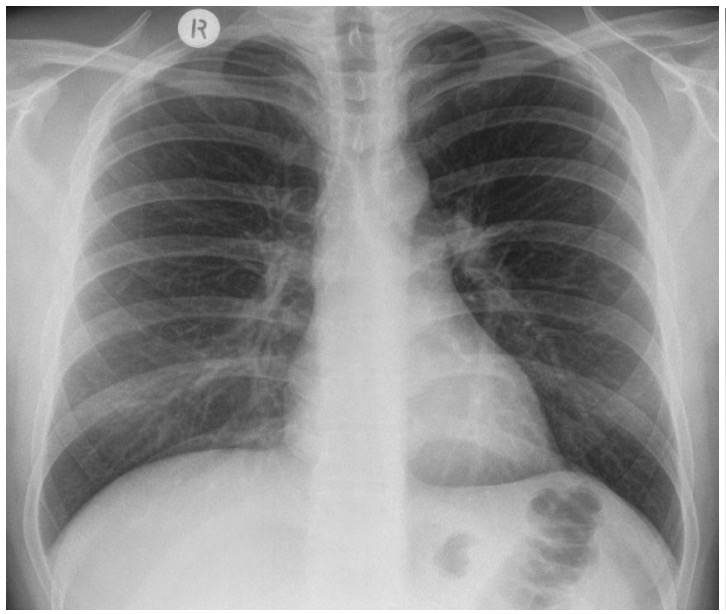
- Chest X-ray
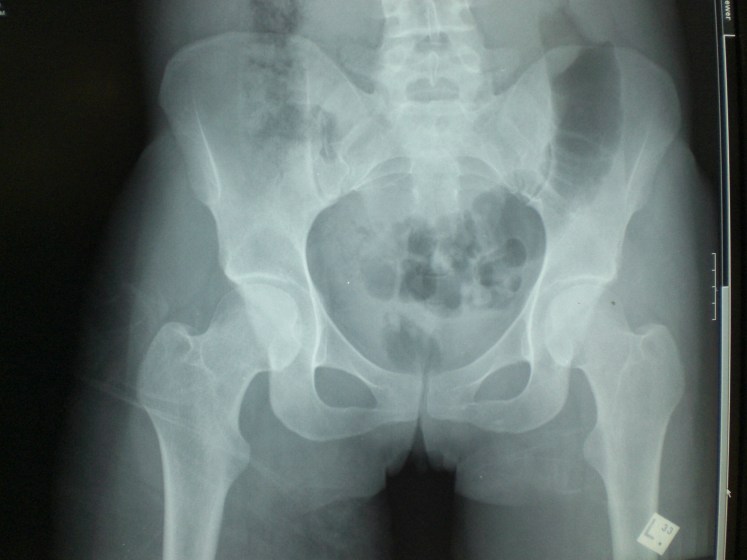
- Pelvis X-ray
- Cervical Spine X-ray – not attended
- Focussed Assessment Sonography in Trauma (FAST) Ultrasound





Secondary Survey and Further Imaging
Main Findings on Secondary Assessment:
- Deformed Left leg (?fractured left femur)
- Multiple grazes on Left leg
- Significant tenderness (on log rolling) in the thoracic spine T10-12
Assessment of the face, head, neck, abdomen, pelvis and chest was unremarkable
Mobile x-ray shows a mid shaft femur fracture:


CT Scanning – Uncomplicated T11 fracture, No solid organ injuries
In-patient Progress
The next day the patient had her femur fixed and post operatively was making an uneventful recovery. However, on day 2 our patient was noted to be increasingly confused with reduced O2 saturations.
The patient’s GCS dropped to 12 and she became agitated.
The O2 sats were 88% on RA.
An urgent CT head and chest was normal.
The patient became anaemic with a HB of 70 with Platelets of 80.
A petechial rash was noted.
What is your diagnosis?
Scroll Down for answer…
A Provisional diagnosis of Fat Embolism Syndrome was made…
Typical Clinical Presentation
Fat embolism syndrome (FES) typically manifests 24 to 72 hours after the initial injuries. However, FES may rarely occur as early as 12 hours or as late as two weeks after a traumatic injury.
Affected patients develop a classic triad (none of which are specific for FES diagnosis):
-
Hypoxia
-
Neurologic abnormalities
-
Petechial rash
Signs and symptoms
- Respiratory Signs (respiratory symptoms are the most common presenting feature of FES).
- Specifically , hypoxia, shortness of breath and tachypnoea are the most common early findings.
- In review of FES patients series 96% of patients with FES were hypoxic
- Subsequently, a clinical picture indistinguishable from acute respiratory distress syndrome (ARDS) can develop.
- Approximately 1/2 of patients with FES caused by long bone fractures develop severe hypoxia (they may require intubation and mechanical ventilation).
-
Neurologic abnormalities
-
Neurologic abnormalities are common. They typically present after respiratory symptoms. Neurologic manifestations include acute confusional state, altered level of consciousness, seizures as well as specific focal neurological deficits.
-
One study reported that mental status changes occurred in 59 percent of patients.
-
- The Petechial rash
- A characteristic petechial rash may be the last component of the triad to develop and occurs in 20% to 50% of cases.
- It is found most often on the nondependent regions of the body including the head, neck, anterior thorax, axillae, and sub-conjunctiva.

A number of other less common manifestations of FES may also be present:
These include anaemia, thrombocytopenia, visual loss (Purtscher’s retinopathy), lipiduria, fever (non-specific), coagulopathy, disseminated intravascular coagulation (DIC) and cardiac complications (e.g. right ventricular dysfunction and hypotension)
Brief Summary
- The pathogenesis of fat embolism is unclear but may be due to fat globules entering the bloodstream following trauma. A systemic inflammation cascade due to circulating fat may lead to the commonly observed clinical picture described above.
- FES typically manifests 24 to 72 hours after the initial injuries.
- The differential diagnosis of FES includes other syndromes cause by embolic phenomenon such as pulmonary embolism (PE) as well as sepsis and ARDS.
- When FES is suspected imaging should be obtained:
- CXR
- CT
- Laboratory studies (e.g. full blood count and coags)
- When FES is suspected imaging should be obtained:
- FES is a clinical diagnosis, and a diagnosis of exclusion
- The classic triad of findings includes hypoxia, neurologic abnormalities, and a petechial rash.
- Less common manifestations include anaemia, thrombocytopenia, fever, lipiduria, and coagulopathy
- No one clinical feature is specific for FES
- There is no definitive treatment except for supportive care. Steroids have been tried with mixed results.
- Most patients with FES fully recover spontaneously but the mortality rate is still reported between 2 and 20% in patients diagnosed with FES

One thought on “A Traumatic Complication”
Comments are closed.