Challenging Cases
Sexual Health and PEP

Case 1 – You are starting your evening shift in the Emergency Department (ED). 32 year old female presents to the ED requesting consideration for “PEP” (Post exposure Prophylaxis) after having unprotected sex with a man from ‘Botswana’. Patient is otherwise well with normal observations.
Case 2 – ‘OSCE Exam Station‘ – Take a history from this 25 year old who presents to the ED with concerns by friends that his is partaking in various risk taking behaviours.
Case 3 – A colleague who has just had a needlestick injury asks you about starting PEP.

Having seen very little in the way of similar cases in the past you are wondering:
- How do we make an assessment for the need for PEP in the ED?
- How do I approach sensitive subjects in my consultation?
- Where do I find the guidelines on PEP?
- How do I get follow up for my patient?
(1) How to make an assessment of a patient in the ED
Specific Assessment in this patient
- In the first instance a thorough history is necessary. Both examination and investigations are guided by your history…
- Allow extra time for the sensitive nature of the conversation
- Prior to starting ensure the following:
- Plan to maintain professional manner and approach
- Don’t rush the consultation
- Prevent interruptions
- Establish Rapport
- Ensure Privacy
- Confidentiality should be emphasised to the patient
- Offer the option of a ‘Chaperone’
- Clear (non-jargon filled) explanations of concepts including risk
- A full and appropriate social history**
- Consider addressing issue of risky behaviour (if appropriate) (e.g. unprotected sex, alcohol or drug abuse)
- Has there been a sexual assault?
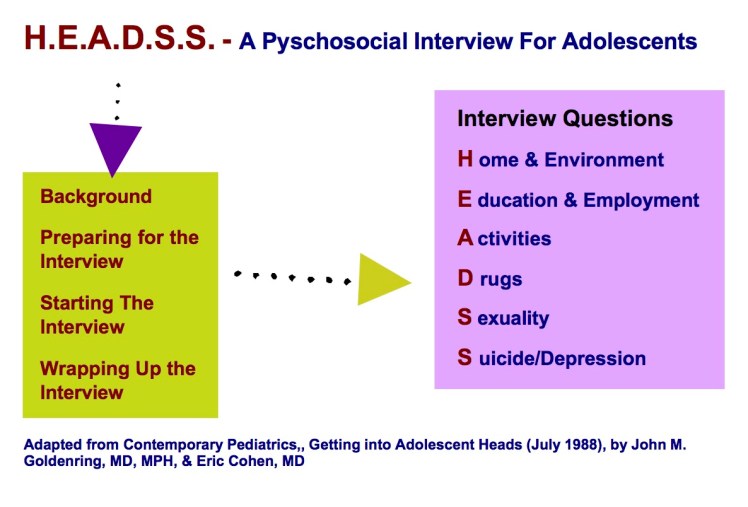
**An alternative may be to use the HEADSS assessment:
- Establish the risk of various communicable diseases:
- (In particular HIV, Hepatitis and other Sexually Transmitted Diseases (STDs))
- Our assessment should be focused on the need for PEP based on the patient’s risk
- Risk of HIV transmission = risk per exposure x risk of source being HIV positive.
- To be effective initiation of PEP needs to occur less than 72 hours after exposure.
- Follow up testing should occur in 3 months regardless of whether PEP is given
- One week testing is no longer recommended
- Emergency contraception and pregnancy
- Ask about pregnancy where appropriate…
- Levonorgestrel 0.75mg stat and 12 hours later, given with antiemetic (it is effective >80% in first 72 hours and warn patient it will delay next period)
- Is STD prophylaxis required?
- Consider given Ceftriaxone 500mg IM/IV or Azithromycin 1g oral after appropirate cultures/PCR testing
(2) Disposition and Follow up
Generally it is wise to contact the local expert (usually an infectious disease physician) if there is any uncertainty regarding the assessment and management for non-occupational exposures. They can guide you on the best options for local follow up.
(3) Where are the new 2016-2017 guidelines?
New National PEP Guidelines (Non-occupational and occupational exposure to HIV)
(4) What are the new features in the National PEP guidelines?
- PEP is no longer routinely recommended for non-occupational exposure when an HIV-positive source has an undetectable viral load
- Tenofovir AND emtricitabine OR tenofovir AND lamivudine are recommended as the preferred 2-drug PEP regimen
- Dolutegravir OR raltegravir OR rilpivirine are recommended as the preferred third agent for 3-drug PEP
- PEP course should be extended by 28 days from the last HIV exposure risk
- PEP is discussed in the context of pre-exposure prophylaxis (PrEP)
- Routine monitoring of blood tests at week 1 is no longer recommended
- Advice has been added to the guidelines regarding:
(5) What about occupational exposure?
- Physicians are more likely to give post-exposure HIV prophylaxis to patients with occupational exposure than nonoccupational exposures with high risk sexual exposure.
- 2% of patients with high risk sexual exposure seroconverted.
- There has not been any documented case of HIV seroconversion from occupational exposure since 2001.
Reference – O’Donnell et al. Missed opportunities for HIV prophylaxis among emergency department patients with occupational and nonoccupational body fluid exposures. Ann Emerg Med. 2016 Sep; 68(3):315-323
(6) How do I convey risk to the patient?
Academic Life in Emergency Medicine (ALiEM) produced the following ‘page‘ to help:

Reference – Vertesi. Risk Assessment Stratification Protocol (RASP) to help patients decide on the use of postexposure prophylaxis for HIV exposure. CJEM : Canadian journal of emergency medical care. 2003; 5(1), 46-8
Alternative Resources

Now I can talk to others about HIV/AIDS more comfortable and w/ the knowledge I got from your training. I am very happy.