Take Homes (8/12/14)

Chest Pain and Risk Assessment
(Louise Cullen – Brisbane)
- Key note address by Dr Louise Cullen
- Chest Pain is a very Common ED presentation with evolving clinical standards
- Appropriate History, Examination and Investigations are required
- ‘High Stakes’ for Missing ACS – historically high mortality in missed Myocardial Infarction
- In the ED the primary goals are judicious EVALUATION and IDENTIFICATION/EXCLUSION of and ACUTE CORONARY SYNDROME (ACS):

According to Dr Cullen – “What we do is art, supported by evidence and tailored to the patient in front of us“
- This was a call to common sense in the work up of the Chest Pain patient in the ED.
- We have to balance the risk in the patient in front of us (and the benefit from admission and investigation) versus the harm of any potential clinical work up of the chest pain.
- I noted on my further reading following this talk that even targeted early Coronary Angiography isn’t guaranteed to improve measurable clinical outcomes (which was a surprise to me). It seems much of the literature quoted for ED use or for guidelines seems to be extrapolated from studies from the 80s and 90s.
- The “Miss” rate acceptable (in surveys) to Australian Physicians was in fact (very interestingly) lower than that of our American and Canadian colleagues. This is despite an apparent less pervasive medico-legal culture down under.

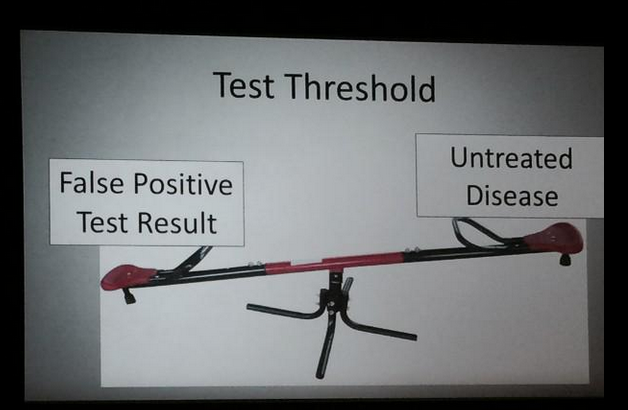
- 2% Rule (Jeff Klein) – Dr Cullen discussed the concept of the Test Threshold and what this means to us.
- Increasing the Sensitivity of our overall evaluation to less than 2% risk is unlikely to provide a useful or beneficial yield for the patient. Indeed further work up may cause harm and lead to iatrogenic complications:
- David Newman – Dr Newman (who unfortunately had planned to speak but was in-absentia from theACEM conference) has argued a case against low yield work ups in low risk patients beyond a troponin in the ED
- However, one important caveat with this approach pointed out by Dr Cullen was that an estimated 1/20 patients ‘ruled out’ after two troponins have important modifiable risk. Therefore, she concludes there is some value in the work up and management of these patients beyond the “ED with troponin rule out” setting.
Reflection on Judicious Further Testing
- We noted after this talk that Dr Newman has never been a fan of Provocative Stress Testing and took away to apply common sense to the individual patient
- He quotes the sensitivity of as Exercise Stress Test (EST) as being much lower that the 70-80% traditionally quoted (by many including me) – around 50% or as he candidly puts it – equivalent to a “coin toss”:

- In Dr Cullen’s Recent MJA review (2013) she states: “Investigations may identify the presence or effects of coronary artery stenosis but, where this cannot be achieved, a broader aim is to further refine risk stratification to identify patients at low risk of an adverse outcome after discharge from the hospital or ED. Exercise stress electrocardiography has become largely obsolete as a means of diagnosing reversible myocardial ischaemia, due to insufficient diagnostic accuracy, but it retains a well established role in identifying patients with chest pain who can safely be discharged from the ED. Exercise stress electrocardiography may be limited by patients’ inability to exercise at an adequate level, non-specific electrocardiographic changes (particularly in the setting of an abnormal resting ECG), and false positive results, but it remains attractive by virtue of its low cost and widespread availability“
Dr Cullen’s Paper Quotes the following sensitivities:

References – (21) Link, (22) Link, (23) Link, (24) Link

Take Home 1
Take Home from this talk – ‘The key is to undertake a judicious work up for the acute chest pain patient with appropriate use of biomarkers in view of the goal accurately identify Acute Coronary Syndrome in the ED’
Chest Pain and Clinical Gestalt
(Anne-Maree Kelly – Melbourne)
- 37,500 Acute Coronary Syndrome Rule outs
- 10-20% of these patients ‘rule in’ for Coronary Artery Disease
- There is a Lower Miss Rates in Larger Hospitals and Academic Centres
- There is a Lower Miss Rate with Exposure to High Risk Patients
- There is a Lower Miss Rate (in the USA) with ‘Board Certified’ Clinicians
- Biomarker Sensitivity has improved – Miss Rates have stayed the same over the last 20 years

- Gestalt has been increasingly sidelined in the Emergency Medicine and in ACS
- Cardiac Risk Factors – They have in fact been found to be ‘futile’ at the individual level
- Jayes et al 1992 – “For a patient presenting to the emergency department, the classical coronary risk factors convey minimal risk for acute cardiac ischemia, especially when compared to the overwhelming importance of the chief complaint and the ECG“
- Han et al 2007 – “Cardiac risk factor burden has limited clinical value in diagnosing acute coronary syndromes in the ED setting, especially in patients older than 40 years“
- Schrock et al 2011 – “This study does not support basing the decision to perform a stress test on the number of cardiac risk factors“
Gestalt and Chest Pain
Historically, clinician gestalt has been shown to be as good as risk scores in the work up of Pulmonary Embolism. There are studies looking into the value of Gestalt in the work up of Chest Pain
Chest Pain Studies:
- Miller et al 2004 – Gestalt (Adjusted) = high sensitivity
- Mitchell et al 2006 – “In a low-risk ED population with symptoms suggestive of acute coronary syndrome, patients with a quantitative pretest probability less than or equal to 2%, determined by attribute matching, unstructured estimate, or logistic regression, may not require additional diagnostic testing“
- Emerging Evidence – Gestalt + ECG + Single Troponin = Close to 100% Sensitivity

- Body et al 2014 – “The Manchester Acute Coronary Syndromes (MACS) rule has the potential to safely reduce unnecessary hospital admissions and facilitate judicious use of high dependency resources”
- RISK SCORES probably are = to GESTALT…
- … but overall Dr Kelly states that neither are enough for ‘rule out’ chest pain patients
- The Cardiology community currently wants a ‘magic bullet’ rule out – they are focused on ACS and seeking more and more sensitive tests. The downside to this aim is a loss of gestalt, no consideration of other diagnosis and false positive results.
- So are Chest Pain pathways the answer? Well, they can be useful, but become out of date quickly and can lead to bias and some cognitive errors. Dr Kelly reminds use to always consider Aortic Dissection, as this is a common cause of death in root cause analyses with most patients going through the chest pain pathway at some stage in their work-up.
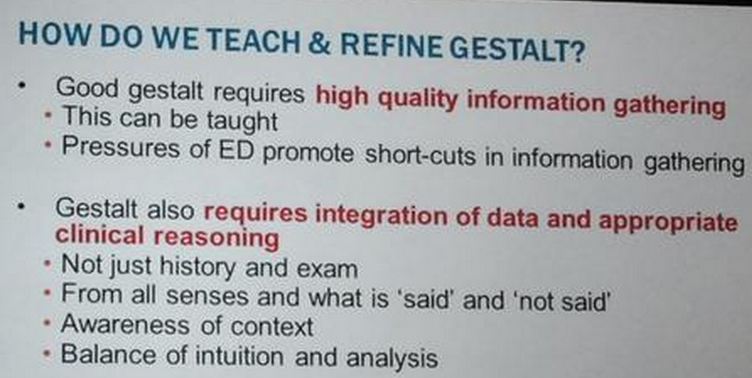
How do we get “gestalt”?
- We are NOT guaranteed to develop good Gestalt with time (our age doesn’t = gestalt so be warned the grey hairs and the no hairs).

- We need to work on clinical reasoning and deliberate practice with feedback
- Gestalt is a skill to be honed and refined…

How do we Maintain our Gestalt?
-
Reflective Practice
-
Case Discussions with colleagues
-
Active Learning
-
Case follow-up (your own cases)
-
Developing awareness of high risk patients
Take Home 2
Take Home from this talk – ‘Gestalt should be re-valued in diagnostic assessments and we need to develop active strategies to refine our gestalt ‘skills’ in emergency training and future professional development’
