

Clinical Toxicology 1
The Approach to the Poisoned Patient (Dr Lau Fei-lung)
- (1) Dose – It’s the Dose “that makes the poison“
- LD50 = Lethal dose that kills 50%
- (2) Patient factors – individual factors that affect the likelihood of toxicity
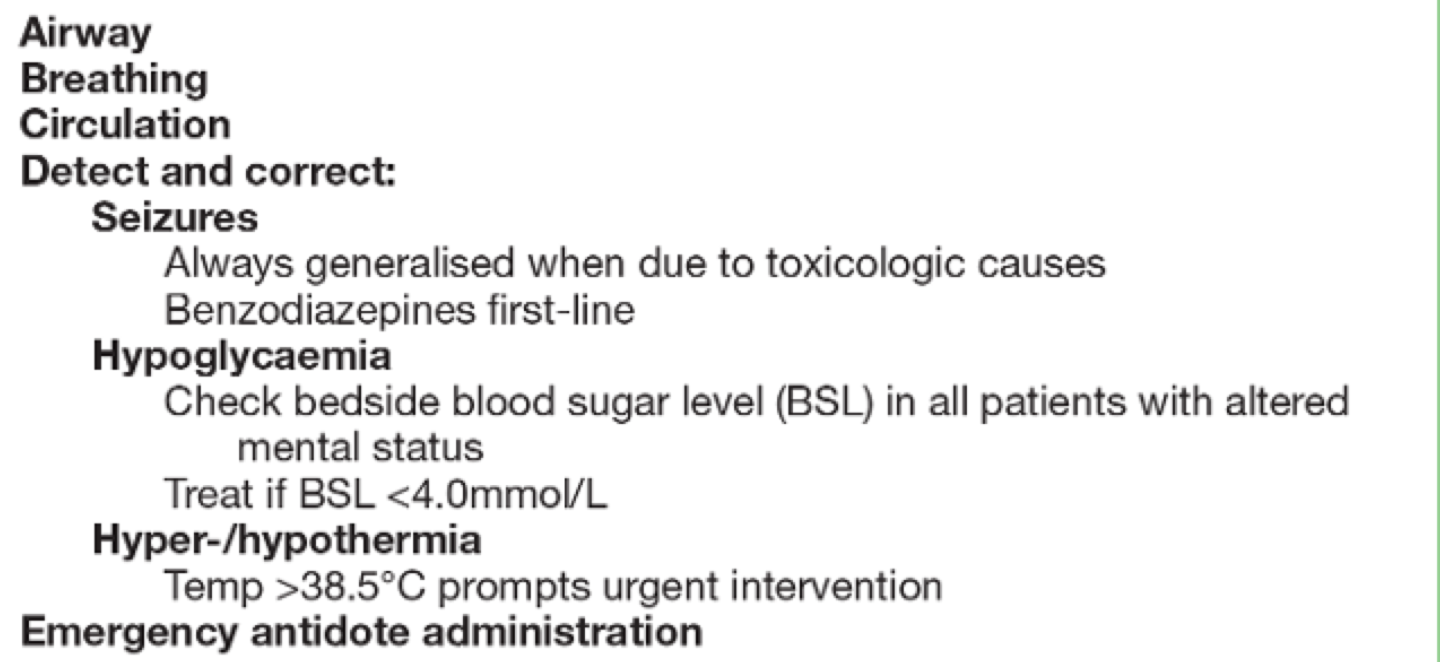
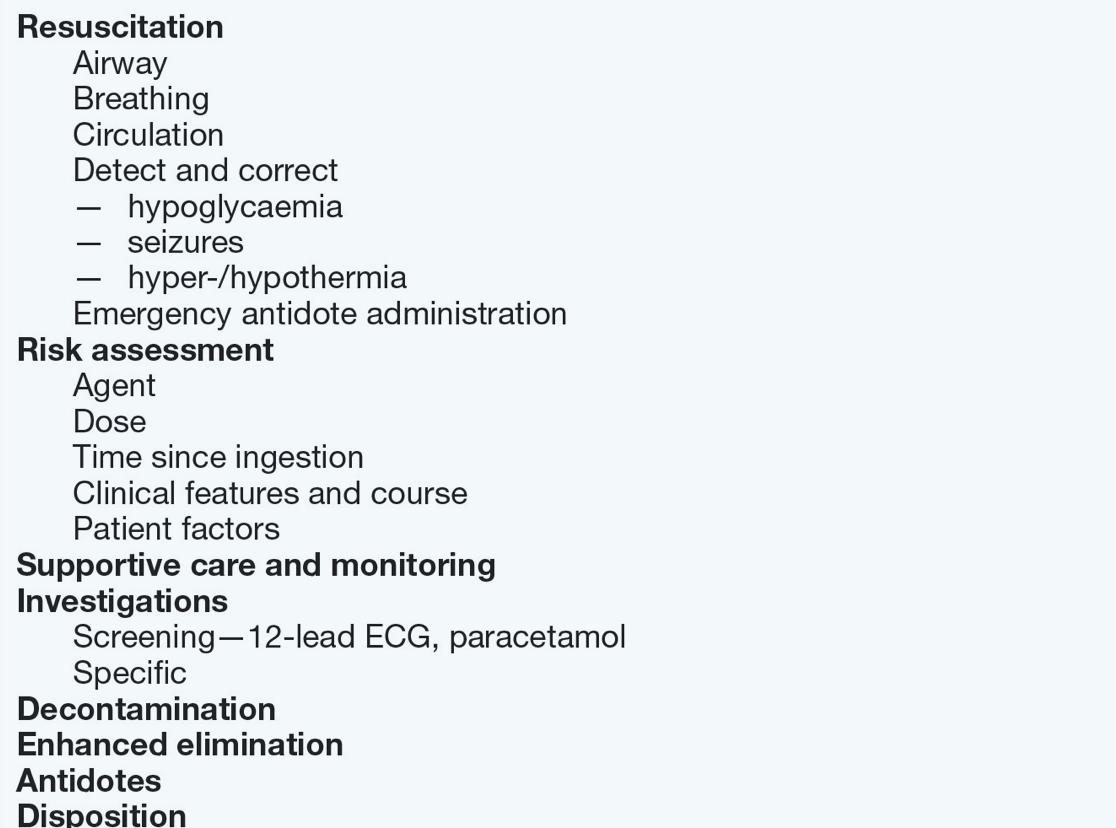
- Resuscitation of the Poisoned Patient
- Self Protection (Universal Precautions) – consider your own safety first
- In the initial phase of management it is important to address the patients “ABC” which may include intubation with mechanical ventilation
- Administration of emergency treatment in the Emergency Department (ED) may be required
- Types of Poisoning
- Accidental
- Self-harm
- Recreational
- Forensic
- Rapid Assessment of the Poisoned Patient in the ED
- History (which substance, which form, how much, when and why)
- Vital Signs (key initiation of immediate intervention in theEmergency Department)
- For Example for Bradycardia remember “PACED“
- Propranolol, Anticholinesterase, Calcium Channel Blocker, Ethanol, Digoxin
- Examination (i.e. pupils, neurological, skin etc.)
- Investigations (ECG, Blood Sugar, Paracetamol Levels, Blood Gas)
- Consider Specific Toxidromes
- Opioid
- Anticholinergic
- Cholinergic
- Sympathomimetic (can be hard to distinguish from Anticholinergic – look for sweating)
- It is important to determine a risk assessment and likely severity of the poisoning:

- Initiate management of the patient based on assessment of risk versus benefit to the patient
- Consult expert help early
- Further Management of the Poisoned Patient
- Specific Treatment and “Antidotes”
- Supportive Care
- Decontamination
- Re-exposure Termination (Enhanced Elimination)

Clinical Toxicology 2
Update on Antidotes (Dr Robert Hoffman)
Overdose has passed Traffic Accidents in term of the number of deaths in the USA
Prescription Opioids and IV Opioids are a major issue – Naloxone is often used as an “Antidote“
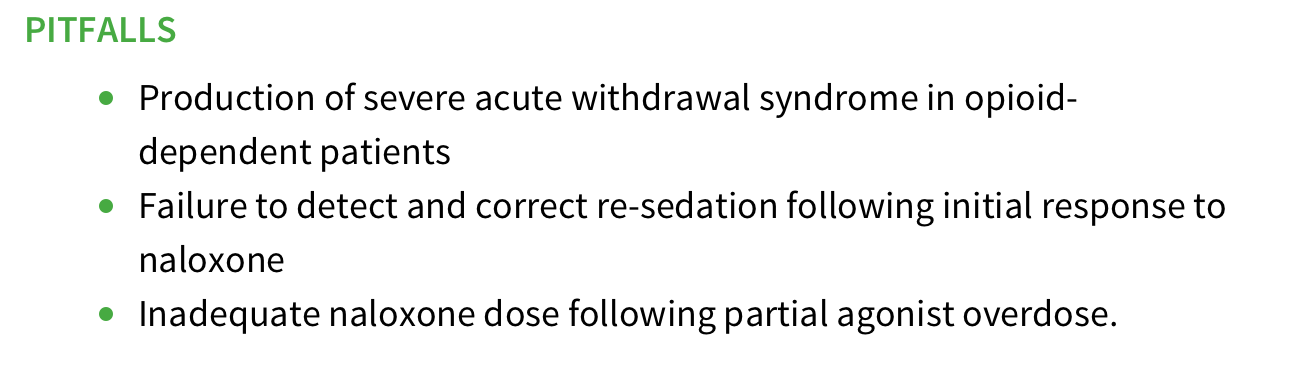
- Naloxone
- Pure competitive antagonist
- The consequence of this is it “does nothing” in those who have no opioids on board
- The drug is very short acting so may required an infusion (give 2/3 of the effective bolus per hour)
- Naloxone doesn’t work oral but is effective by multiple other routes (IV, SC, IM, trachea, nasal)
- Avoid or reduced the dose for Opioid Dependent
- Dr Hoffman suggests 0.05mg IV unless impending respiratory arrest in the dependent patient
- Large doses have been associated with Acute Respiratory Distress Syndrome (ARDS)
Anticholinergic Syndrome can have a wide variety of causes – some consider Physostigmine the antidote
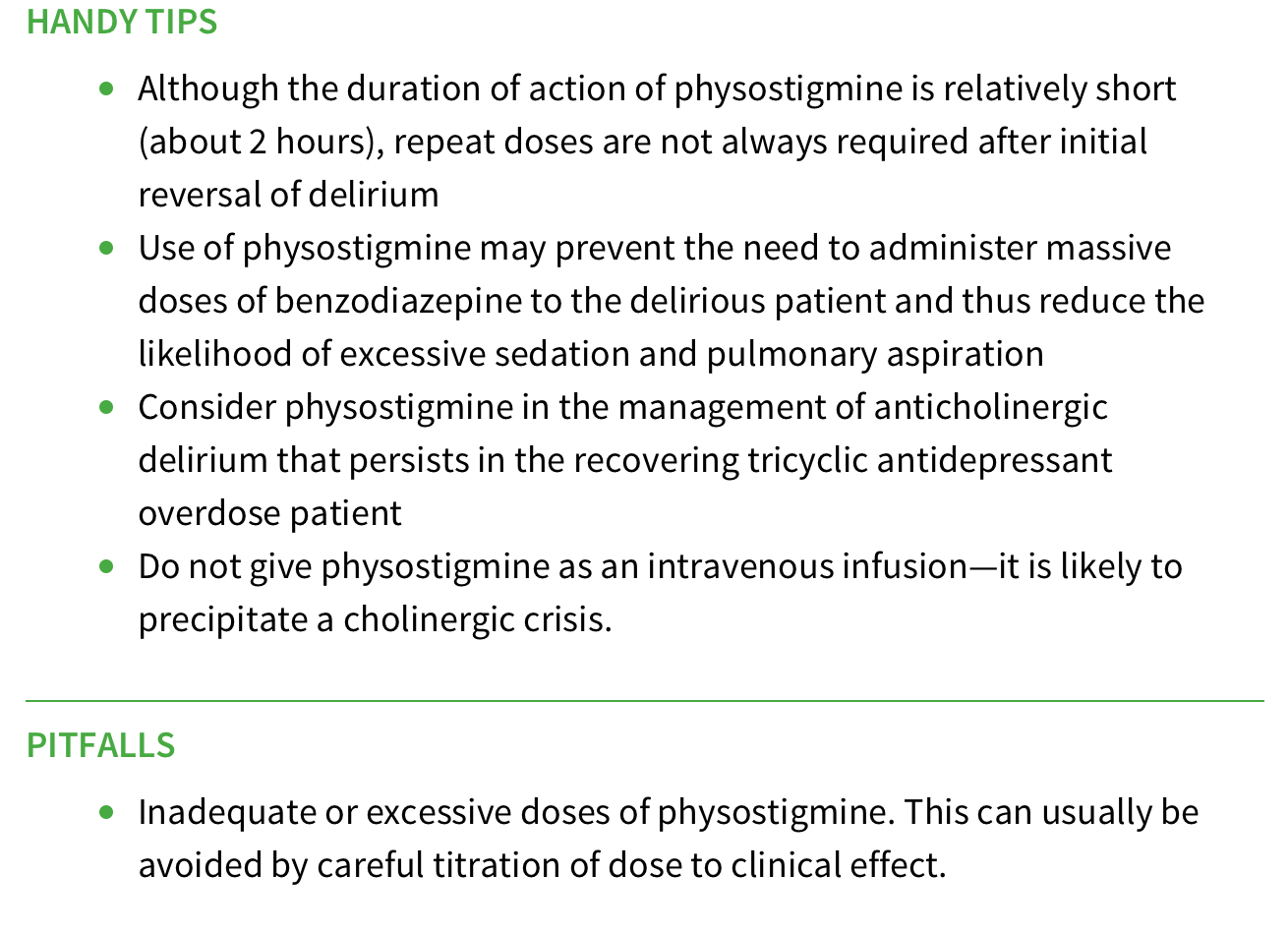
- Physostigmine
- A good ‘reversal agent’ for anticholinergic syndrome – many toxicologists are reluctant to give
- Not a competitive antagonist – increases acetylcholine – will make anyone cholinergic and therefore can have significant side effects
- Case reports in the 1980s suggested significant cardiac toxicity – however, this was in the context of aberrant ECG findings and mixed overdoses
- More recent studies (retrospective) favour its controlled use
- If we are going to use this we need
- a relatively normal ECG
- slow infusion (over 5-10 minutes)
- any cholinergic effects or patient back to normal should trigger you to stop
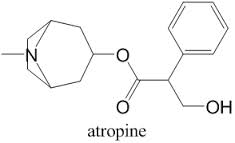
Organophosphates – massive issue in developing countries
- Atropine
- Reversal of Muscarinic Symptoms
- Dose – it is suggested that we start relatively high with our Atropine dosing and double the dose every 3-5 minutes (does over 32mg are often required)
- End Points – Drying of Secretions (don’t worry about pupils)
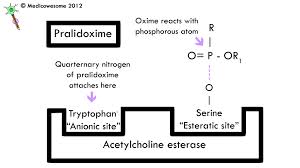
- Praladoxime
- Shown to work in the “test tube” environment – can reactivate the Cholinesterase enzyme in the lab
- In human studies significant contradiction in two studies
- The case for –
- The case against –
- Using the treatment – not for “bolus” – will cause acute weakness

Cyanide – rapidly acting poison (rarely survive to hospital)
- Cyanide blocks the last step in oxidative phosphorylation
- = catastrophic effect on energy metabolism
- = rapid death
- Various Antidotes
- Sodium Nitrite – can be effective but drops BP
- Thiosulphate – can be effective but a risk of Methhaemoglobinaemia
- B12 – ‘Hydroxocobalamin’ – mops upCyandide 2.5 -5grams IV – first choice in USA
- Can be given with (in addition to) Thiosulphate
- Causes Red Urine, Red Skin etc.
- ‘Everything turns red‘ (warn nurses and the lab!) – this will have a significant effect lab results (troponin, creatinine) as well as the pulse oximeter and COHb
Methaemoglobinemia
- Methhaemaglobinaemia
- Methylene Blue – can be an effective therapy
- G6PD – is not contraindication or reason for failure of this treatment (the speakers cited issues with 1970s case report by Rosen et al that has created a myth that the treatment is ineffective in the absence of NAPDH – in fact the poisoning caused a reduction in the levels of NAPDH)
Clinical Toxicology 3
Decontamination (Dr Robert Hoffman)
‘Appears to be Common Sense‘
Lavage, Charcoal and Bowel Irrigation should be effective (at least in theory)
In reality mixed results in literature
- Ipecac – not recommended by the ICEM conference speakers (for use in developed countries)
- Gastric Lavage – this area is a controversial issueamoungst toxicologists
- Dr Hoffman and the other ICEM speakers disagree with the “position statements” of the Clinical Toxicologists “never to use Lavage”
- They believe that early lavage may be used selectively
- Of note, a paper by Li Yi in 2009 suggested that early lavage in critically unwell poisoned patients in China resulted in a reduced mortality but the authors did not conclude that lavage was indicated
- A massive Colchicine overdose, chemotheraphy OD or lethal Aspirin OD would be examples of overdoses when Dr Hoffman and the other speakers would consider Gastric Lavage
- Activated Charcoal – multiple studies showing benefit in various scenarios – “charcoal is not dead”
- QT in Citalopram
- Yellow Oleander (Sri Lanka)
- Paracetamol Poisoning
- Stomach emptying speed is really quite variable – and may be slower in large overdoses.
- Time is an issue but don’t always use one hour as a cut off!
- Juergens et al showed benefit up to 4 hours so Charcoal should be considered beyond 1 hour in selected patients
- Whole Bowel Irrigation
- a good way to “alienate your nurses” – but can be used in specific circumstances:
- Consider in large metal (e.g. iron) overdoses and sustained release drugs
- a good way to “alienate your nurses” – but can be used in specific circumstances:
- Enhanced Elimination (EE)
- Dialysis – effective with drugs of small molecular weight, lack of intracellular binding, low protein binding and low volume of distributions
- The Extracorporeal Treatments in Poisoning Workgroup (EXTRIP) – currently looking at evidence
- Indications may include – Aspirin OD, Severe Paracetamol OD, Lithium OD, Carbamazepine OD, Methanol OD,
- No evidence in TCA and a variety of other toxins – the results of the EXTRIP analysis will be published in the coming months to help us rationalise the use of EE and dialysis
