
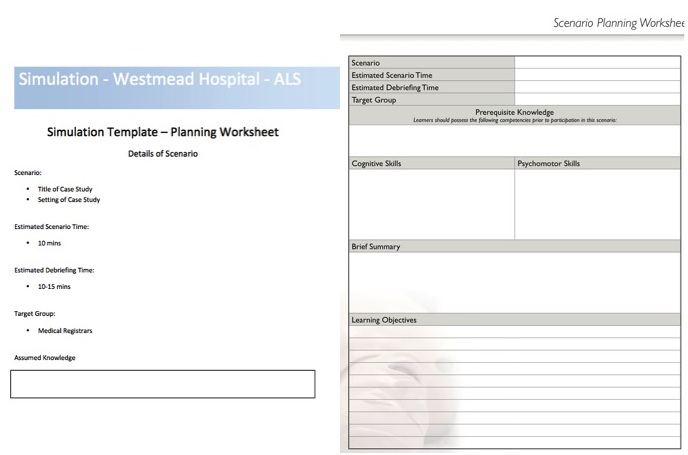
- What are the Definitions of ‘Simulations’ and ‘Simulators’?
- Simulation
- Simulation is an Educational Technique
- Allows the student to gain an emotive and immersive learning experience.
- Allows the recreation of a clinical experience without risk to patients.
- Simulator
- A device that attempts to create characteristics of the real world environment.
- Simulators vary from basic Part Task Trainers to complex Full Body Manikins with Complex Simulation Software that can produce excellent haptic feedback and a high degree of fidelity for the learners.
- Why has Simulation developed as a major teaching technique in healthcare?

- What communication strategies can be learned and taught through Simulation for use in Time Critical Emergencies?
- Convey Information
- Strategy for Best Results:
- Be Technically accurate and Specific in use of language
- Strategy for Best Results:
- Co-ordinate the Team
- Strategy for Best Results:
- Use CRM and have and effective team leader
- Strategy for Best Results:
- Team Cohesiveness
- Strategy Best Results:
- Develop a healthy team climate.
- Train together
- Use team member names
- Pre-brief and debrief
- Strategy Best Results:
- Disagreements within the Team
- Strategy for Best Results:
- Negotiation
- Strategy for Best Results:
- Listen to and Address Concerns within in the Team
- Possible Strategy:
- Graded Assertiveness
- Use C.U.S.S:
- I am CONCERNED about the Oxygen level falling and lack of ETCO2
- I am UNSURE that we can be sure if the ET tube is in the right spot as I observing that there is no ETCO2, tube fogging and that the stomach looks bigger.
- This is a SAFETY issue – the patients saturations are rapidly falling
- STOP – this patient needs to be ventilated with a BVM and then re-intubated
- Graded Assertiveness requires the team leader to tell the team this is okay and that there will be no adverse circumstances as the result of questioning actions
- Possible Strategy:


Harvard Crisis Resource Management Review
- Why use simulation?
– Simulation, by providing a representation of a real world experience, fits with the principles of effective adult education (adult learning theory). David Kolb and Donald Schonn developed the concept of ‘Experential Learning‘:

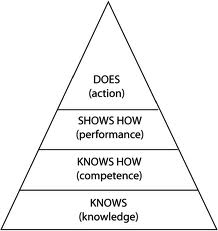
– Developing Competencies requires the learner to build on past knowledge and practise problem solving (Miller’s Pyramid):
– Simulation may be helpful in developing training and assessments for new undergraduate and postgraduate programs. In particular, Work Based Assessments (WBA) and Entrustable Professional Competencies (EPA).
- What are the PROS and CONS of using Simulation?
PROS
-
Patient Safety
- Scenarios protect patients.
- They do this by improving teamwork and communication as well as avoiding exposure of patients to ‘practice’ by very junior staff and students.
- Good for Uncommon Scenarios (exposure to rare events in simulation may been the only access in terms of training)
- Good for Common Emergencies (Link – Team Drills of Emergencies such as Cardiac Arrest)
- Scenarios protect patients.
- Skills Training
- Rapid Acquisition of Skills
- Opportunity for Drill
-
Team Training
-
Curriculum and Convenient Timing
- Standardised Scenarios presented to all learners
- Adult Learning
- Reflective and Experential Learning (see above)
-
Assessment
-
Recertification and Continuous Professional Development
CONS
-
Expensive (dollars to establish a centre and maintain the facility)
-
Negative Transfer
- Due to simulation lack of fidelity or debriefing
- Non valid application of Technique
- Lack of Trained Staff
- Lack of Equipment
- Adequate or Appropriate Fidelity

Development of Simulation in Medicine:
- 1960s Laerdal: ‘Resusci-Annie’ Simulator
- 1967: SIM ONE Simulator
- 1987 CASE 1.2 at Stanford University (Med Sim Eagle)
- 1990s – 2000s
- METI Human Patient Simulator (HPS)
- Laerdal SimMan – cheaper version of HPS
- Increasing Training and Education in Simulation
- Literature on the effectiveness of Simulation
- High Fidelity Simulation
- Hybrid Simulation
- Patient Based Simulations (Simulated Patients)
- Part Task Trainers
- Computer Based Simulation
- High fidelity simulation involved the use of life like mankins to create realism in scenarios.
- Fidelity can be:
- Environmental (simulation area should look like a hospital and have similar equipment)
- Physical (haptic feedback and life like features of the manikin)
- Psychological (degree of immersion in scenario)
Types of High Fidelity Manikin and Approximate Costing
- METI Man HPS (CAE) – Unit Cost >$200,000
- SIM MAN 3G – Unit Cost $96,000
- Mega-code Kelly – Unit cost $11,000
- SIM MAN Essential – Unit Cost $20,000


- Patient Focused Simulation
- Standardised Patients
- These can be used in High Stakes Assessment but there are Cost and Training Issues
- Professor Nestel at Monash is an expert in this area:
- Standardised Patients
- A variety of manikins representing body parts are commonly used for training:




- Pause and Discuss
- Probably best used for simple emergency proceadures (e.g. Pacing) orsmall groups who are new to simulation
- +/Δ
- Plus Delta Model of Debriefing: rapid pointing out of gaps in learner’s knowledge and skills by debriefer

- Advocacy Enquiry
- Also known as the Harvard Debriefing Method
- Essentially making the debrief into a puzzle to unravel…
- Go over what they did well…
- Go over what the facilitator thinks would be an alternative (not necessarily better) approach
- Key phrase – ‘I am Curious’ about what you were thinking when you did this (specific)
- Can you help me understand what was happening?
- Pendleton’s Rules of Debriefing
- What went well?
- What could have gone better?
- What do you think of this?
- General Tips
- Follow the team into the room and listen to their conversation
- Assess the learners frames (the basis of knowledge and experience behind their actions)
- Give the learners space
- Address serious safety issues with the learner (privately) and speak with senior faculty about the best approach
- Short term benefits seem to be reproducible but patient quantantive outcomes as a result of simulation are hard to quantify with high level evidence.
- Cost Effectiveness Unclear.
- Applying existing clinical guidelines in a high fidelity simulation environment can be used for training and learning as well as potential assessment and revalidation of health care workers
EBM References
- Weller J, Robinson B, Larsen P, Caldwell C. Simulation-based training to improve acute care skills in medical undergraduates. N Z Med J 2004; 117:
- Grantcharov T et al. Randomized clinical trial of virtual reality simulation for laparoscopic skills training. Br J Surg 2004; 91: 146-150.
- Weller J et al. Simulation in Clinical Teaching and Learning. MJA 2012; 196 (9) 594



Further Reading
(1) Harvard Debriefing – Harvard Debrief
(2) Simulation Overview – Simulation Overview


A further useful link for Graded Assertiveness – http://www.impactednurse.com/?p=5453
http://resus.me/on-chicken-bombs-and-muppets
This is an amazing post. Ruthlessly efficient!