ABDOMINAL PAIN CASE 2
‘That doesn’t look right’
You have been asked to review a 67 year old male patient called Jim. He has presented to the Emergency Department with abdominal pain after passing a large amount of meleana per rectum.
Further, he has a history hypertension and gout. At the bedside you note that he looks pale.
The vital signs are: HR 120 (sinus), BP 80/40 and resp rate 26, Sats 94%. After a copious vomit (which has the appearance of haematemesis) the nursing staff move the patient to the resus bay and place him on 02 in the left lateral position. The registrar working on the floor today has requested two units of packed cells.
Whilst waiting for the blood to arrive, which of the following should be prioritised?
Choices:
- Position patient prone
- Optimise temperature, acidosis and coagulopathy
- Prevent hypercarbia
- Order APTT
Commit to an answer and scroll down
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
Correct Answer = “2” (Optimise temperature, acidosis and coagulopathy)
A take home message:
General supportive measures remain consistent in all resuscitation scenarios, especially in the bleeding patient. Warming patients may help prevent worsening coagulopathy and further bleeding.
Some more information:
The lethal triad in significant trauma or severe haemorrhage is:
- Hypothermia
- Coagulopathy
- Acidosis
These three factors all cause, and contribute to, acute coagulopathy of trauma/shock (ACoTS) which leads to further bleeding in the context of an existing major bleeding issue. This patient’s presentation is consistent with an upper gastrointestinal bleed with signs of haemodynamic instability (tachycardia and hypotension). This should be thought of as a life-threatening bleed. Loss of blood leads to reduced oxygen delivery to tissues and so supplemental oxygen should be immediately provided.
It is important to explore the patient’s background history to find potential sources of bleeding and management which commonly include: peptic ulcer disease and oesophageal varices. Other causes include angiodysplasia, malignancy, coagulopathy (especially NOACs).
Coagulopathy can be optimised by reversing anticoagulation (e.g. warfarin), warming the patient and providing a balanced transfusion (ratio of packed cells to FFP of 1:1). A blood warmer should be used.
Local practice varies but typically transfusions are a balanced combination of FFP, cryoprecipitate and packed cells with smaller volumes of platelets. Calcium should also be measured and replaced as the ionised (blood gas) calcium level is below 1.0mmol/L.
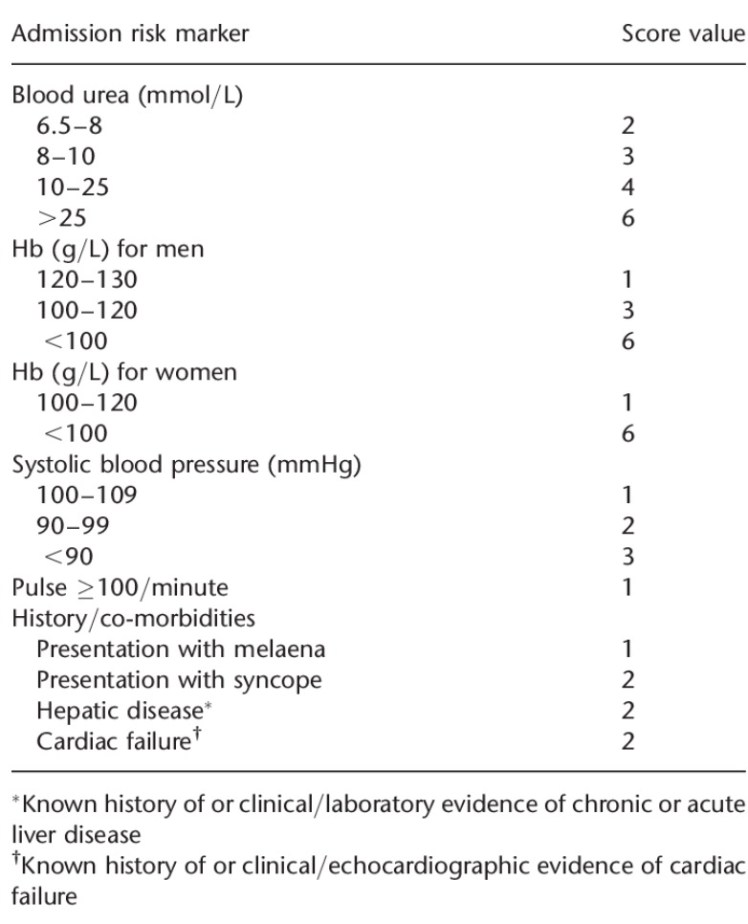
One method of stratifying the ‘severity’ of the presentation is the Glasgow-Blatchford score. (Low risk = Score of 0 / Any score higher than 0 is higher risk for requiring transfusion, endoscopy, or surgery):
Links and References:
- The Lethal Triad – https://lifeinthefastlane.com/ccc/major-haemorrhage-in-trauma
- The Glasgow Blatchford Score (GBS) – https://www.aci.health.nsw.gov.au/networks/eci/clinical/clinical-resources/clinical-tools/gastroenterology/upper-gi-bleeding/upper-gi-bleeding-risk-scoring-systems
- A summary of upper GI bleed management – https://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0004/395131/Emergency-Management-of-Upper-Gastrointestinal-Haemorrhage-Flowchart.pdf
- An extensive podcast review of GI bleed emergencies – https://emergencymedicinecases.com/gi-bleed-emergencies-part-1
Follow our EMIG page here – https://goo.gl/jNi6Dh
