![]()
AMEE 2016 Barcelona – Highlights
This year was my first AMEE conference and I wanted to jot down some shorthand reflections on the experience. AMEE is short for the ‘Association for Medical Education in Europe’. It is a big organisation and has a reputation for high quality meetings.
I couldn’t not make the ‘AMEE 2015‘ meeting in Glasgow but have always had this conference on my bucket list as a budding but somewhat novice clinical educator…




So where do you start after a week like this?
The medical education community is clearly going strong on the basis of the 3,500 delegates from over 80 countries.
Plenaries were led by speakers from developing countries as well as by medical students – refreshing for a scientific meeting of this size. Additionally, students were both seen and heard in the symposium conversations which was also encouraging.



On the down side there were some archaic components of note. WiFi (an essential part of modern medical meetings) was snail pace slow and audio-visual deficiencies continually distracted the speakers and learners.
Twitter was busy with healthy discussion but there was a notable lack of comment about the Free Open Access Medical Education (#FOAMed) revolution. In fact there was a complete absence of reference to ‘FOAMed’.
The ‘AMEE Live‘ streaming has the potential to increase the reach of this conference but its cost may be a limiting factor for those wishing to access conference content remotely…
Regardless of these minor gripes, the overall ethos and learning opportunities generated were positive.
My AMEE virgin and educator novice perspective is that this is an inclusive international meeting. What was apparent were the large number of younger speakers, faculty gender mix and a general absence of death by power point.

Top Ten Learnings from Barcelona
I’d like to share a ‘top ten‘ ten learning experiences from AMEE 2016 for my benefit and hopefully for your interest:
(1) PechaKucha and the Singing Haematologist
PechaKucha is a simple presentation format where the presenter of the lecture shows 20 images for 20 seconds each. The images advance automatically and the presenter talks along to the images.
These talks can be recorded on a screen at home or presented live. It’s fresh way to get really punchy 6 minute talks into a big scientific conference and it worked well at AMEE!


The PechaKucha format was invented by Astrid Klein and Mark Dytham and kicked off in Tokyo in the early 2000s. It has now grown to be a movement on a par with the TED talks.
Meanwhile the ‘fringe‘ sessions at AMEE saw the star of the show being a British haematologist living and working in New Zealand. He uses his creative talents to break up his lectures with entertaining (and informative) musical interludes:
(2) Use of Videos to Teach ‘Non Technical’ Skills
The pre-conference workshops led by Copenhagen Academy for Medical Education and Simulation (CAMES) and Dr Walter Eppich highlighted some pearls for using medical simulation:
- (a) Learning from the Movies
- Directors like Alfred Hitchcock are expert in showing what you need to see as the viewer. In the same vein, when creating a simulation event we need to take control of the experience for the learners. Immersion in the experience for the participant(s) can create learning opportunities. In a medical simulation you can use anticipation and limited information. Giving participants a phone call with a pre-hospital notification with limited information can provide an opportunity for preparation and richness of learning in the debriefing.
- (b) Anticipation – ‘Anticipation’ is a great area for discussion in simulation. Revealing limited information in a timely & sequential fashion can be really effective.
- What strategies can you see in this video that were used to create an effect?
- (c) Leadership – consider watching videos to highlight the importance of leadership with your colleagues. Compare and contrast the following examples:
- Video 1 – Click Here
- Video 2 – Click Here
- Video 3 – Click Here
(3) Debriefing
- Learn through talk:
- In the debriefing consider use of the PEARLS framework:

(4) A Simulated Clinic?
Dunedin (NZ) and Keele (UK) use ‘SECO‘ clinics for teaching consultation skills to students. This could be tailored to specific objectives and extrapolated to many settings.
Improving confidence, patient safety and communication are obvious benefits with cost and training actors being significant barriers. The key factors include:
- Unobserved, true-to-life patient encounters in a simulated general practice
- Open access to resources (texts, internet, or phone advice from a senior colleague)
- Student control of time management for the duration of the clinic
- Formative and summative assessment which aligns assessment, clinical teaching, learning, and future professional practice
- Focus on the outcomes of the consultation

(5) Blended Classrooms and Use of Technology (without a budget)
There are loads of technologies out there to create a flipped classroom.
Simple online resource development without a massive budget may not as far away as you think. 3 new tools stood out as potentially fit for purpose:
- Pinion (i-phone and i-pad) – Click Here (email for login)
- MIT App Inventor – Click Here
- Learner Designer – Click Here

(6) Coaching and Feedback
A central theme of the conference was increasing our skills in coaching and feedback.
The theme with feedback which resonated with me included:
- Feedback should ideally be based on direct observation:
- The caveat is that observation is often viewed as “performance altering” by the learner – this may jeopardise the experience and pose a significant barrier to quality feedback…
- ‘Credibility’ and ‘Constructiveness’ are essential in giving high quality feedback
- There should be existing healthy long standing relationship between the ‘assessor’ and ‘learner’
- The person giving feedback should ideally not be the direct supervisor
- The sole purpose is to improve performance with no summative assessment(s) tied to the feedback
We need to improve our feedback culture in medicine!
Could we take influence from other domains such as sports?
- Deep Dive – Dr Atul Gawande discusses the path the excellence in this article:
(7) Competency Based Medical Education
Is clearly an area of controversy worldwide. Cynical delegates stated that ‘Competency Based Medical Education’ (CBME) could be misinterpreted as ‘Checklist Based Measurable Education’.
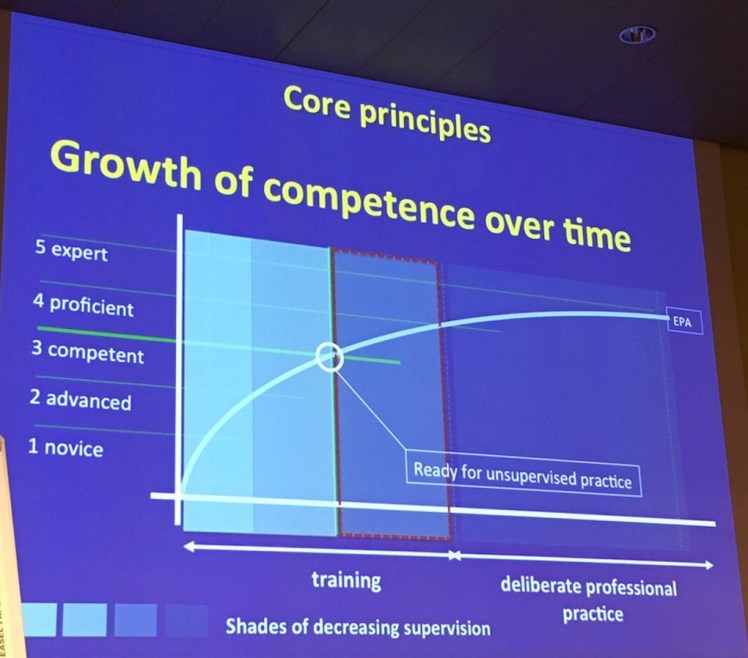
At AMEE the question was posed do you want to be treated by a competent doctor or an excellent doctor? Clearly the level of competency needs to be set a particular level and may take some learners longer to achieve than others…
CBME is a very confusing concept to the newcomer or novice educator (me) but is nicely explained by lovely academics in the Netherlands.
I noted a lot of tension at AMEE between the idea of striving for excellence versus aiming competence… Pose yourself the following question… Which one of these ‘competent‘ pilots do you want to land the plane?




(8) Gaudi and The Sagrada Familia
The Barcelona church known as the ‘Sagrada Familia‘ was designed by genius and pious architect Antoni Gaudí (1852–1926). The church is still not complete after over a hundred years due to its magnificent proportions and a long hiatus in building during the 20th Century under the Spanish dictatorship of General Franco.
Building was started in 1882 and only the crypt and entrance was completed at the time when Gaudi died. It is due to be completed at the present rate in 2026…
Gaudi died a hero in 1926 although I learned this week that he was run over by a tram and left in the street as a ‘tramp’ before finally receiving help several hours later when he was recognised.
The pictures below shows the combination of natural light, art nouveau and gothic influence:



(9) The ANTS System for summarising medical ‘non technical skills‘
Dr Rhona Finn and colleagues have previously described a really nice summary of the essential non technical skills that optimise patient safety in the operating room and beyond. I have previously used David Gaba’s list of ‘crisis resource management’ skills but think this model summarises things really nicely for a critical care setting:

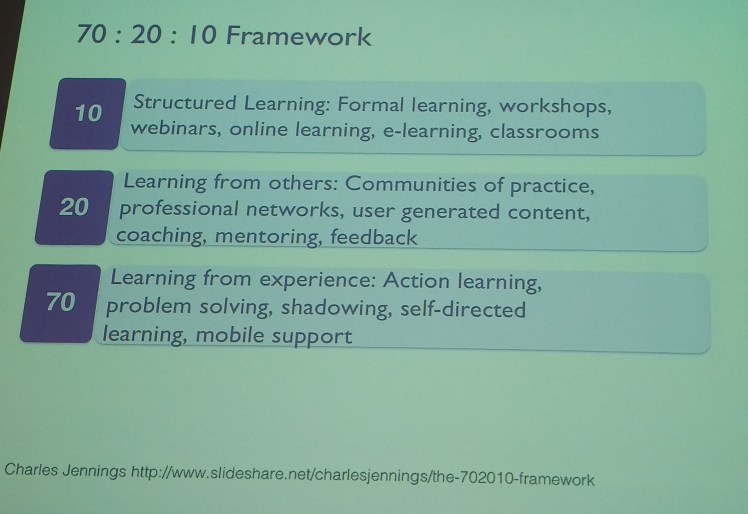
(10) 70 : 20 : 10
Is the lecture dead? Maybe not completely, but the idea we need the right ratio of teaching methods came through at AMEE 2016. The ‘70 20 10 rule‘ describes a ratio of balanced teaching modalities.
It may be something to consider when designing new programs for adult learners:
Take Home
Old Wisdom – Striving for excellence in teaching in 2016 is an inspirational challenge but sometimes old wisdom shines through.
This model from Robert Gagne in 1965 seems to apply 50 years on:


One thought on “Pearls from the AMEE 2016 Conference”
Comments are closed.