Background
Over 95% of the total body potassium content is intracellular. The amount of potassium in the body is regulated by renal glomerular filtration and tubular potassium excretion. The steroid hormone aldosterone which enhances renal secretion of potassium.
Other factors which can affect renal excretion of potassium include sodium excretion in the kidney, dietary potassium intake and plasma pH. Potassium has many biological functions including nerve conduction and muscle contraction.
Hyperkalaemia
- Defined as of more than 6.0 mmol/L
- A ‘Time Critical Emergency’
- Always think of “pseudohyperkalaemia” (haemolysis)
- Potassium secretion is proportional to flow rate and sodium delivery through distal nephron (diuretics will cause Low K
- Acidosis is associated with worsening
- Most medical treatment in the ED is temporising
- Urgent Dialysis may be required
Causes
- Pseudohyperkalaemia
- Crush Syndrome (trauma) and/or release from cells (transfusion)
- Excess Intake
- Decrease Excretion (renal)
- Medications
- Drugs that change potassium movement across cell membranes
- (e.g. β blockers, Digoxin, Potassium-containing drugs)
- Drugs that reduce aldosterone
- (e.g. ACE inhibitors; Angiotensin II blockers, NSAIDs, heparin, transplant drugs)
- Drugs that inhibit aldosterone binding to the mineralocorticoid receptors
- (e.g. Spironolactone, Trimethoprim)
- Drugs that change potassium movement across cell membranes

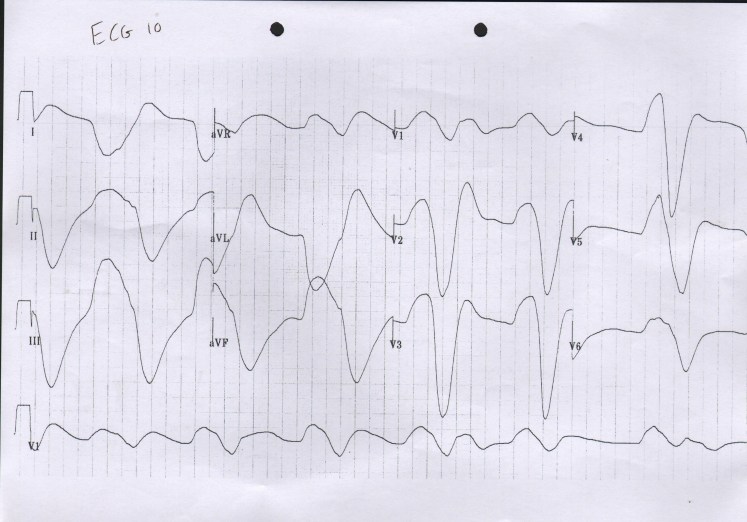
ECG
First Action – Monitor your patient and obtain an ECG
- The classic ECG changes are not always present in true High K
- Progressive changes include:
- Flat/long P waves
- Broad bizarre QRS complex
- Slurring into the ST segment
- Tall tented T waves
- Long PR interval
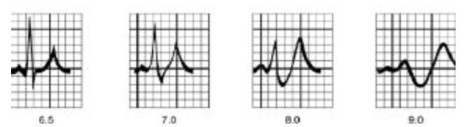
- In severe cases – sine waves, ventricular fibrillation, progressive heart block, asystole
Management Priorities
RESUSCITATION
- Call for assistance and assemble an appropriate team (nursing and medical). Move the patient to the Resuscitation Bay.
- Attach the patient to 3 lead ECG telemetry and observe with continuous non-invasive monitoring
- Apply O2 / salbutamol
- Position Patient – Sit patient up
- Obtain IV access
- Send repeat bloods (including a bedside point of care VBG)
- Start Intravenous (IV) fluid (e.g. 0.9% saline 500ml/h if not known ‘renal patient’ or a significant risk of fluid overload with small amounts of IV fluid) – this is safe and appropriate in almost all patients
SPECIFIC TREATMENT
- Immediate 12 lead ECG
- Stabilize cardiac membrane using Calcium
- Shift K+ into cells
- IV insulin 10 units
- 25-50 grams glucose (e.g. 50mls of 50% dextrose)
- Check the blood sugar and assess the patient for neurological symptoms within 20 minutes
- Nebulise Salbutamol (e.g. 10mg nebuliser)
- If acidotic/critical – consider 8.4% sodium bicarbonate
- 50 ml of 8.4% solution over 10 minutes
- Remove K+ from system
- In patients with adequate renal function – IV Frusemide 1mg/kg (40-80 mg)
- Calcium Resonium / K Binding Resin – possibly very ineffective and risk of complications (see below)
- IV normal saline solution for volume expansion if dry, crush syndrome or DKA
- Definitive treatment for High K is haemodialysis
- Monitoring – do follow up ECGs and continuous telemetry
- Document the patient needs ‘Low K+ Diet’ & ‘Fluid Balance Plan’
- Admission under renal team / ICU
Summary of Treatment Options
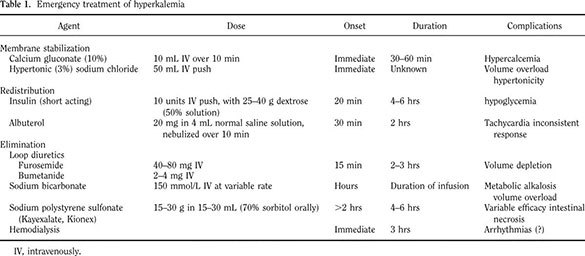
Weisberg et al. Management of Severe Hyperkalemia. Crit Care Med. 2008 Dec;36(12):3246-51.
- Calcium Therapy
This will NOT lower the total body or serum potassium levels but will reduce the risk of arrhythmia
- Calcium is indicated if there are any ECG changes or evidence of cardiac instability. Consider in any patient with a K greater than 7.0
- Calcium gluconate: Give 10ml of a 10% solution over 10 mins
- Calcium chloride is often used (can lead to thrombophlebitis)
- Use calcium with care in patients on Digoxin (controversial) as there are historical reports of patient deterioration


Lowering the K and Dialysis
Insulin and Dextrose are effective but temporary treatments. Dialysis is the gold standard for removing potassium. This can provide immediate and reliable removal. Only use 8.4% Bicarbonate in acidotic patients.
Calcium Resonium
- ‘There is Dubious Evidence for the use of this Drug‘
- The resin was invented in the 1950s for industrial purposes and then someone had the idea of putting it in patients colons to exchange cations and hence bind potassium (mostly absorbed in the colon).
- Scherr et al (NEJM):
- This paper did show a drop in K
- In the study there were 32 patients
- They had Binding Resin +/- a laxative,
- Most patients had glucose, insulin, low K diet and bicarbonate therapy
- THERE WAS NO CONTROL GROUP
- In the end in this study 23 /30 patients had a decrease of at least 0.4 in their K value… This was cited as evidence of effectiveness However, there was no control, and a lot of HCO3 / Insulin was used
- A second paper in the same journal:
- also studied the use of binding resins with only 10 patients in the study
- One small study in 1998 showed no change in serum potassium concentration after a single dose of binding resin or placebo (both with and without a sorbitol additive)
- The authors concluded – “Because single-dose resin-cathartic therapy produces no or only trivial reductions in serum potassium concentration, and because this therapy is unpleasant and occasionally is associated with serious complications, this study questions the wisdom of its use in the management of acute hyperkalaemic episodes.”
Further Resources
- Handout – Acute Hyperkalaemia
- Podcast – Update on HyperK Management
- Paper – ECG unreliable (Montague et al)
- Podcast – EM-Crit Podcast 32
- Debate – Binding Resins
