The Art of Presenting in Healthcare

The Power Point Presentation
(Sydney Medical School – updated)
PDF – CLICK HERE
PPT – CLICK HERE

Key Points
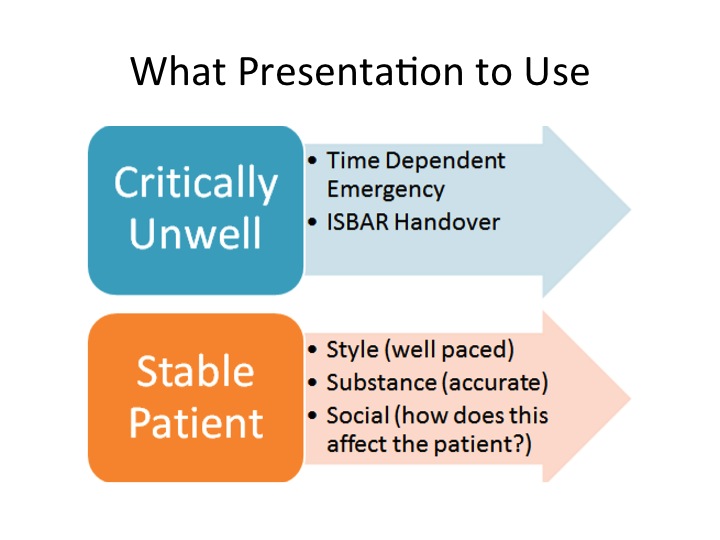
- Your style of presentation depends on:
- The Acuity of the case
- The Urgency of the possible diagnosis and management
- The Environment (e.g. Out-patient v Theatre)
- The Listener (e.g. Surgeon v Medic)
Presenters and Listeners have many different Styles of presenting a case.
All healthcare professionals have individual styles and your presentation and listening skills need to be tuned to the person you are talking too.
In general there are 4 types of communicator roaming around most hospitals:
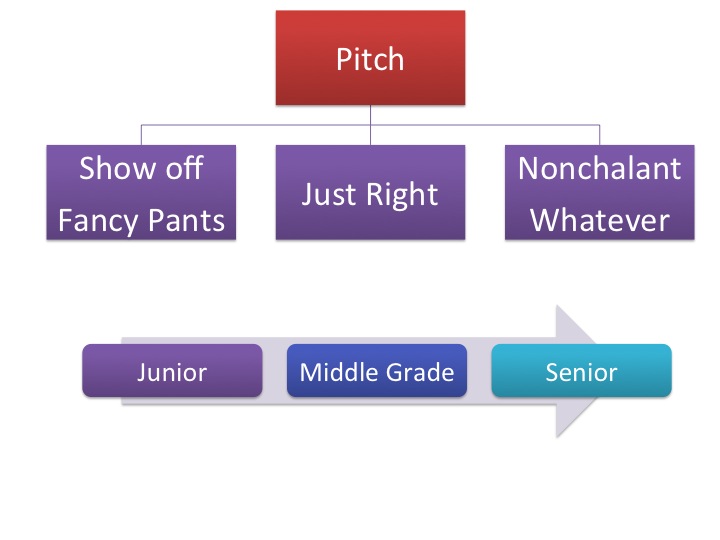
‘Pitch’
Pitching your presentation at the right level can be difficult.
This is a challenge whether you are senior or junior:
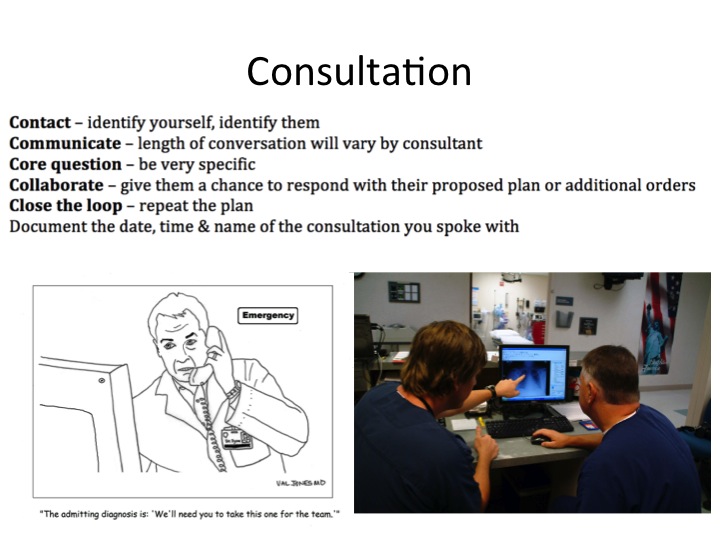
Consultation Skills (Obtaining a Consult)
When your Consult or discuss a case use the 5 “Cs” and use ISBAR (see below) to structure your handover:
Tools – ‘ISBAR’
ISBAR Examples
Poor
Improving
Good
Closing the loop of communication is a key consideration. What does this mean?

Closed Loop Communication Video 1
Closed Loop Communication Video 2
Presenting Short Cases
- Doing this well is all about having your examination or history taking skills refined to the point where you don’t have to think about the next step (automated).
- This allows you to have a well-paced, stylish and considered presentation
- Notice in the following example from the UK MRCP examination the excellent body language, tone of voice, cadence and case synthesis:
Presenting Long Cases
- Top Tip – Your powers of observation are really important. Have a good overview of the patient before your get too fixated on the details of the patient’s complex medical history.
Overview
- Give the patient TIME – they will tell you their problems and you can write them down
- Try various methods of GETTING THE INFORMATION DOWN – i.e. Pens, Paper and various Templates
- You have a LONG TIME – use the time wisely
- Practice OPENING STATEMENTS and closing statements as much as possible as this is where the money is:
- Practice using a refined version of the ISBAR handover
- Seek FEEDBACK from experienced registrars or consultants
- Quality PRACTICE with examiners under actual exam conditions
- Do at least 10 good cases under time pressure
Structure
Like any good story your long case should have a beginning a middle and an end.
Opening Statement
- Top Tip – the phrase “in more detail” allows you to pause and give the examiners (and you) time to relax into the main part of your presentation
Middle Section
End (Summary of the Case)
Your “issues for discussion” can be either “Diagnostic“, “Management” (or both).
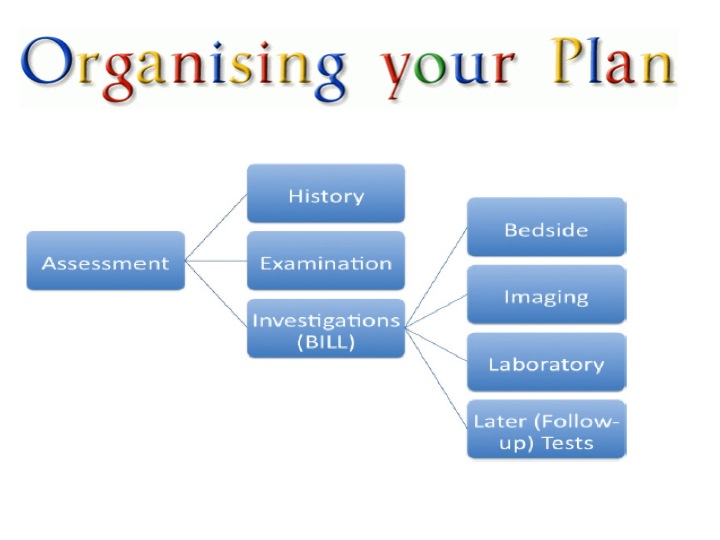
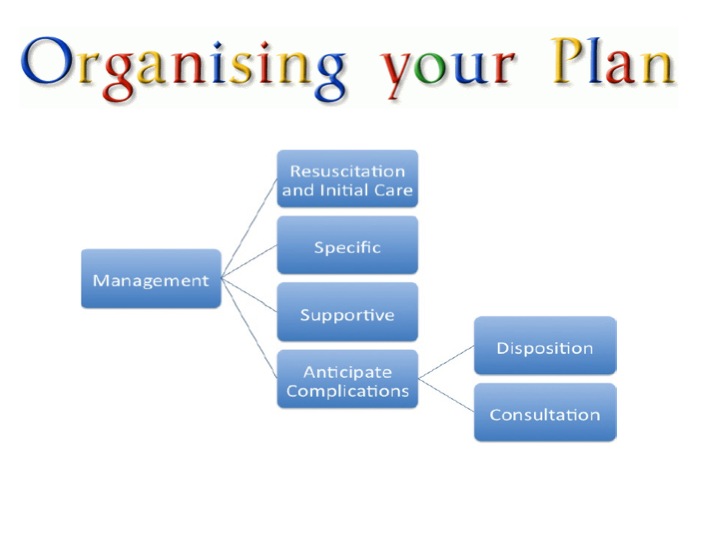
How do you best organise these?
The answer is Structure.
For example for Investigations consider ‘BIL‘: Bedside, Imaging and Labs as groups rather than FBC, CXR and ECG as a list.
It is most impressive when you have a clear and organised structure:
Summary
- In an Emergency / Time Dependent Situation:
- Use I.S.B.A.R.
- Be Concise
- Emphasise Life Threats
- Consider Management and Investigations as simultaneous activities
- Use Graded Assertiveness if you are concerned
- In a Long Case:
- Be Structured
- Have a Story (Beginning, Middle and End)
- List your Issues
- Diagnostic
- (and/or) Management
- Have a Holistic Approach

Another Great resource in this regard is FOAMed from REBEL-EM – http://rebelem.com/how-to-call-a-consult/