
Nepean Hospital Trauma Day (12/11/2014)
The Institute of Trauma Management (ITIM) education evening took place at Nepean Hospital in New South Wales today.
Among the highlights were a focus on the Spectrum or Traumatic Brain Injury (TBI), Local Police Information, Simulation Training and Pre-hospital Trauma Care. We present a very short review of key points and take homes.

Traumatic Brain Injury (TBI)
Dr Andrew Davidson – Neurosurgery
- GCS Mnemonic – Remember for “EVerMore” – ‘E’ ‘V’ ‘M’ = 4 5 6
- Eyes (E) out of 4 – Verbal (V) out of 5 – Motor (M) out of 6
- Overall outcomes not improving in last 10 years for Severe Injuries (Roozenbeek et al)
-
TBI – Severe Injury = GCS 3-8
-
TBI – Moderate Injury = GCS 9-13
-
TBI – Mild Injury = GCS 14-15
- Invasive Intracranial Pressure (ICP) Monitoring Controversial as South American Study showed no difference in mortality with use of the ICP monitoring. (NB: As I recall the control group got regular CT scans that may have biased this study)
- Dr Davidson recommends ICP monitoring in most cases of significant TBI and this is the local practice in my experience.
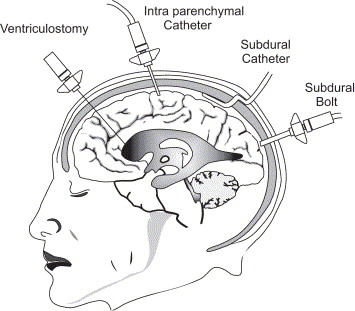
 Dr Davidson recommended Ventricuostomy as opposed to other methods of ICP monitoring as it allows for therapeutic draining as well as pressure monitoring.
Dr Davidson recommended Ventricuostomy as opposed to other methods of ICP monitoring as it allows for therapeutic draining as well as pressure monitoring.
- Excellent Guidelines onTBI recommended by Dr Davidson included:
- Brain Trauma Foundation (BTF)
- Neurosurgical Society of Australia (NSA) – Rural Management
- Institute of Trauma Management NSW (ITIM)
- Poor evidence for most phamaco-therapies (e.g. steroids, statins and magnesium).
- Limited evidence of routine hypertonic saline or mannitol although is sometimes used in the ED and pre-hospital in selected cases.
- Limited evidence for invasive surgery but this is used selectively by many Neurosurgeons
- Areas of future interest include the role of Hypothermia which has shown promise in small paediatric studies (NB I note that it has been disappointing in adults and larger studies to date)

Minor Brain Injury
Sharryn Byers – CNC
- Minor Brain Injury is commonly sporting related
- Overall 1,000,000 presentations to ED a year in the USA
- Prevention is a key part of any management strategy
- All head injuries (including minor knocks) should be taken seriously
- There is an association with multiple injuries and poorer long-term outcomes

- On going studies in Rugby Union
- In particular there are on going studies into head guard equipment
- No clear evidence at this stage of benefit
- There is an association with reduced musculature athletes being at increased risk of head injury in Rugby
- In particular there are on going studies into head guard equipment
- Football (Soccer) Studies
- Heading the ball in soccer may also be an impact injury an with multiple repetitions and long-term harm.
- Reduced impact from newer ball designs
- Concussions on Field
- Consider using the ‘SCAT 3’ – Sports Concussion Assessment Tool
- Includes a Maddock’s Score
- SCAT 3 should be completed by a Medical Officer
- Essentially this is a series of short-term memory tests
- Consider using the ‘SCAT 3’ – Sports Concussion Assessment Tool

- Post Traumatic Amnesia (PTA)
- Short term memory dysfunction can last from hours to months post injury. PTA is common after mild head injury.
- Length of any ‘PTA’ may be more important than the length of Loss of Consciousness at the scene.
- Full PTA is required if patients fail an abbreviated PTA test
- 15% of patients with normal CT scan may have significant concussion symptoms a year after their injury
- Patient Discharge Advice – Head injury advice cards are available in up to 7 languages from the ITIM site: www.aci.health.nsw.gov.au/networks/itim/clinical/trauma-guidelines/Guidelines/head_injury_cpg/discharge_advice
Colonic Injuries
Dr Aldenb Lorenzo – Senior Registrar
- Classic dogma from World War 2 suggested than patients should have a stoma.
- There appears to have been a change in management of penetrating Traumatic Colonic Injuries
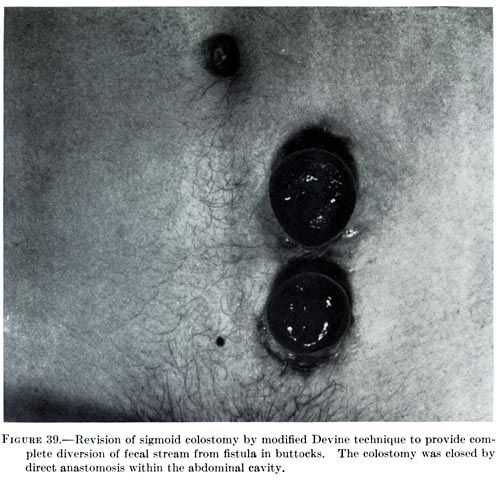
- Dr Lorenzo looked at these injuries retrospectively (over a ten-year period) at his hospital
- 55 patients were included in his study:
- Knife was the most common weapon (56%) and Gun Shot (33%)
- An increasing number of patients had a primary repair through the study’s course.
- Rates of stoma use went down over the time of the study.
- Transverse Colon was the most common site of injury.
- Higher Grade Injuries were more likely to have a resection or diverting ostomy
- Dr Lorenzo suggests a future multi-centre prospective study on Colonic Injuries
Crash Investigation – Police Department
Sergeant Brett Samuels – NSW Police
- Crash Investigation Unit (CIU)
- CIU covers severe and near fatal (Grievous Bodily Harm (GBH) or fatal accidents in the state of New South Wales.GBH injuries upheld in court has included compound fractures, skin burns, serious scarring and according to Sergeant Samuels any injury requiring anaesthetic in-hospital.
- Punishable Offences range from Long Prison Terms to Fines:
- Manslaughter – 25 years in prison
- Aggravated Dangerous driving – death 14 years
- Aggravated dangerous driving – GBH – 11 years
- Dangerous Driving – 10 y years
- Dangerous Driving causing GBH – 7 years
- Negligent Driving causing Death – 18 moths
- Negligent driving causing GBH – 9 moths
- Traffic and minor offences – fines
- Punishable Offences range from Long Prison Terms to Fines:
- CIU covers severe and near fatal (Grievous Bodily Harm (GBH) or fatal accidents in the state of New South Wales.GBH injuries upheld in court has included compound fractures, skin burns, serious scarring and according to Sergeant Samuels any injury requiring anaesthetic in-hospital.
- CIU are acting on behalf of victims and therefore require some degree of non-specific information about the patient’s condition. Major Crash Investigations take 3-9 hours to complete. While privacy is obviously important some information can help move on an investigation and avoid closing major roads for prolonged periods of time.
- There is a legal basis for the police seeking information under local jurisdiction (Section 18 under limits on disclosure of personal informal 1998).
-
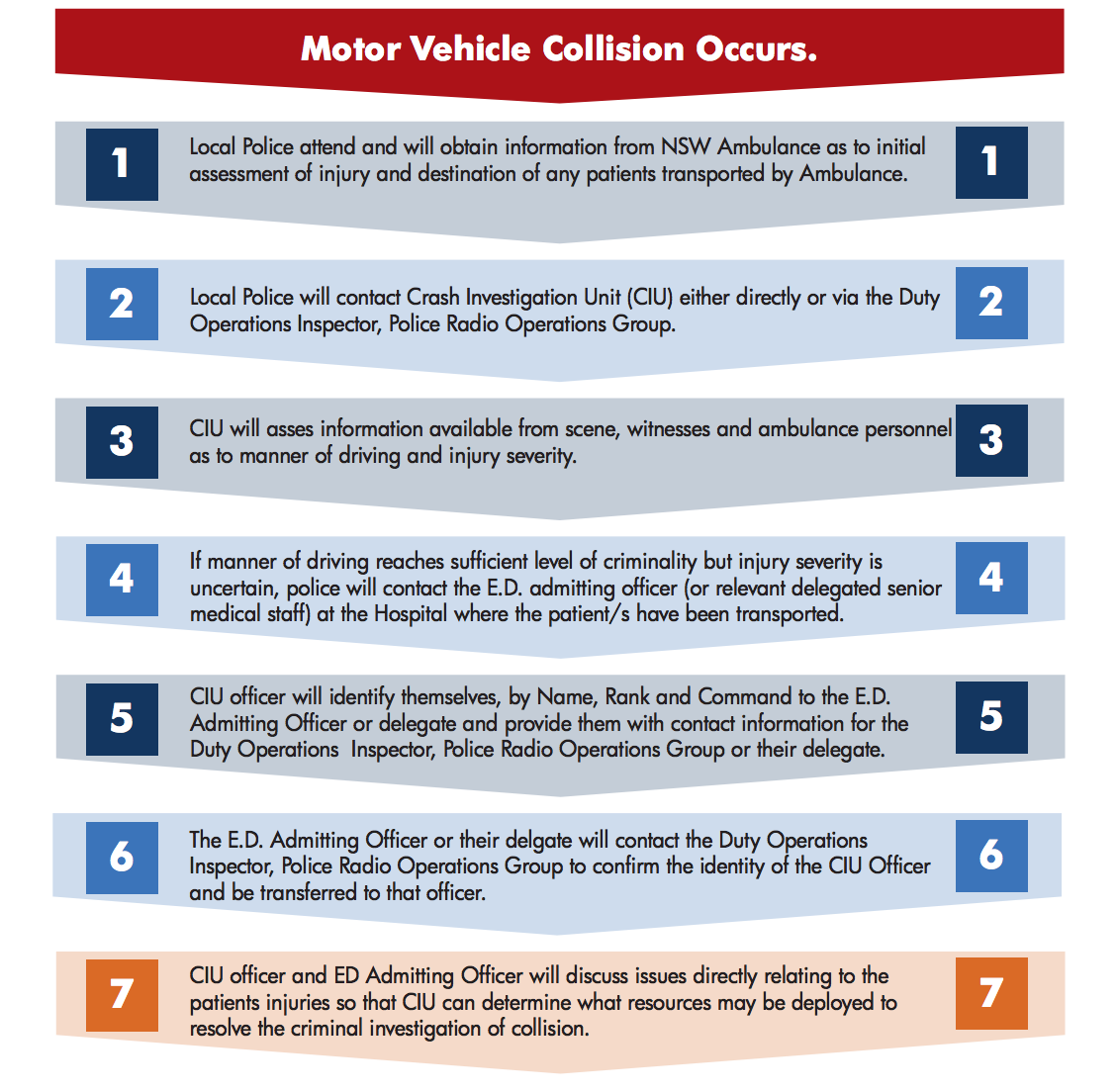
Key Point – CIU Recommend that the hospital should share information.
Summary is found on the following 7-step flow chart:
- Police Blood Alcohol sample – should be taken within 12 hours but preferably within 2 hours.
- If on a stretcher patient’s ONLY require blood.
- If brought in by police they need blood and urine within 4 hours
- Getting this “wrong” can lead to failing to convict dangerous drivers
- For police statements sufficient details is important (more detail means less likely to have to go to court contrary to popular belief).
- It is important to preserve evidence (even seemingly trivial) as much as possible – even paint fragments and glass have been used to convict driving offenders
Trauma Team Training
Lizzie Barrett and Emma Jarvis – Nepean Hospital Senior Educators
- Trauma Team Training is an increasingly popular and widespread course in NSW trauma centres
- Long standing course originally run at the North Shore Simulation centre
- Now being rolled out across the state – encouraged by ITIM
- Updates and course materials will soon be available on the ITIM website in order to run the course from scratch in both low and high fidelity sim centres


- The Nepean Hospital team have taken on a four-hour model with immersive high level simulation training
- BEnefits include – patient safety, teamwork and crisis management skills
- Barriers include costs and buy-in from local departments
- Each individual department need to be responsible for training individual doctors and nurses in their respective roles
- Future directions may include a full run through sim from pre-hospital to ED thought to CT scan and to theatre
Case Presentations
Dr Shane Trevithick – Helicopter Hero
Pre-hospital Lessons
- Head Injury Management
- Avoid Hypoxia
- Avoid Prolonged Hypotension
- Selectively use Hypertonic Saline (mannitol is not suitable for the pre-hospital environment as it is crystallised at cold temperatures)
- Rapid Sequence Intubation (RSI) in selected cases – this can reduced the time to definitive management in hospital (may take time at the scene but saves MORE time in the Emergency Department)
- Application of the “best the hospital has to offer” to the pre-hospital environment is an essential component of retrieval medicine. Working in retrieval challenges your assumptions as you get to see medical practice in a variety of locations.
- Team Training
- A well-trained small team can be as, if not more, efficient than a larger hospital team



- Use Checklists (in the hospital as well as in the pre-hospital environment)
- Have a Standardised Approach in your department
Helicopter Heroes Videos:
